Andreou Anna P, Efthymiou Maria, Yu Yao, Watts Helena R, Noormohamed Faruq H, Ma Daqing, Lane David A, Crawley James T B
Centre for Haematology, Imperial College London, London, United Kingdom; Section of Anaesthetics, Pain Medicine & Intensive Care, Imperial College London, London, United Kingdom.
Centre for Haematology, Imperial College London, London, United Kingdom.
PLoS One. 2015 Apr 1;10(4):e0122410. doi: 10.1371/journal.pone.0122410. eCollection 2015.
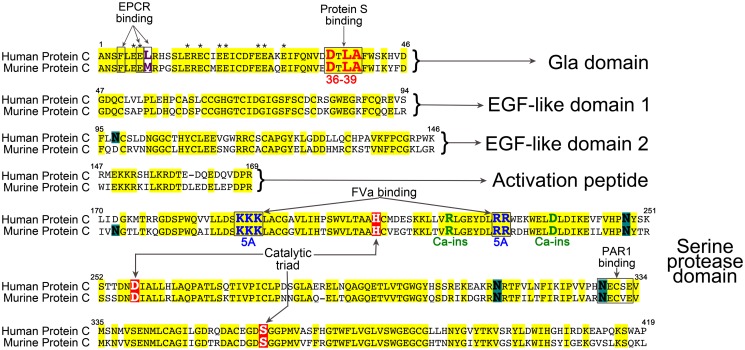
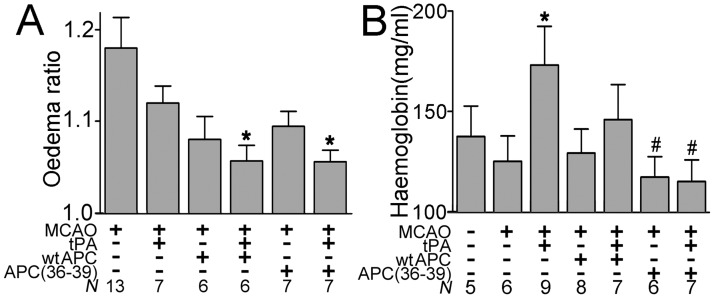
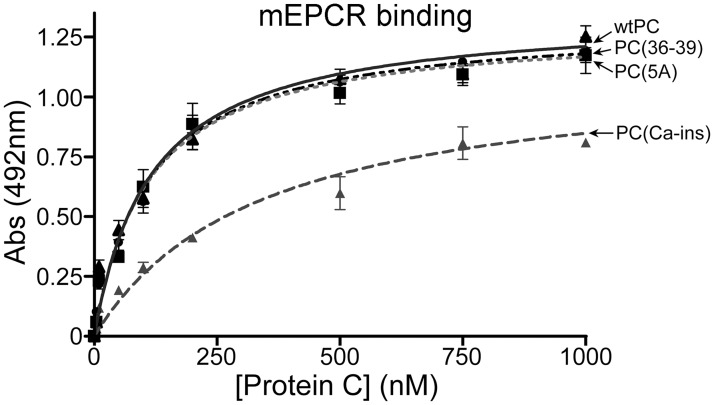
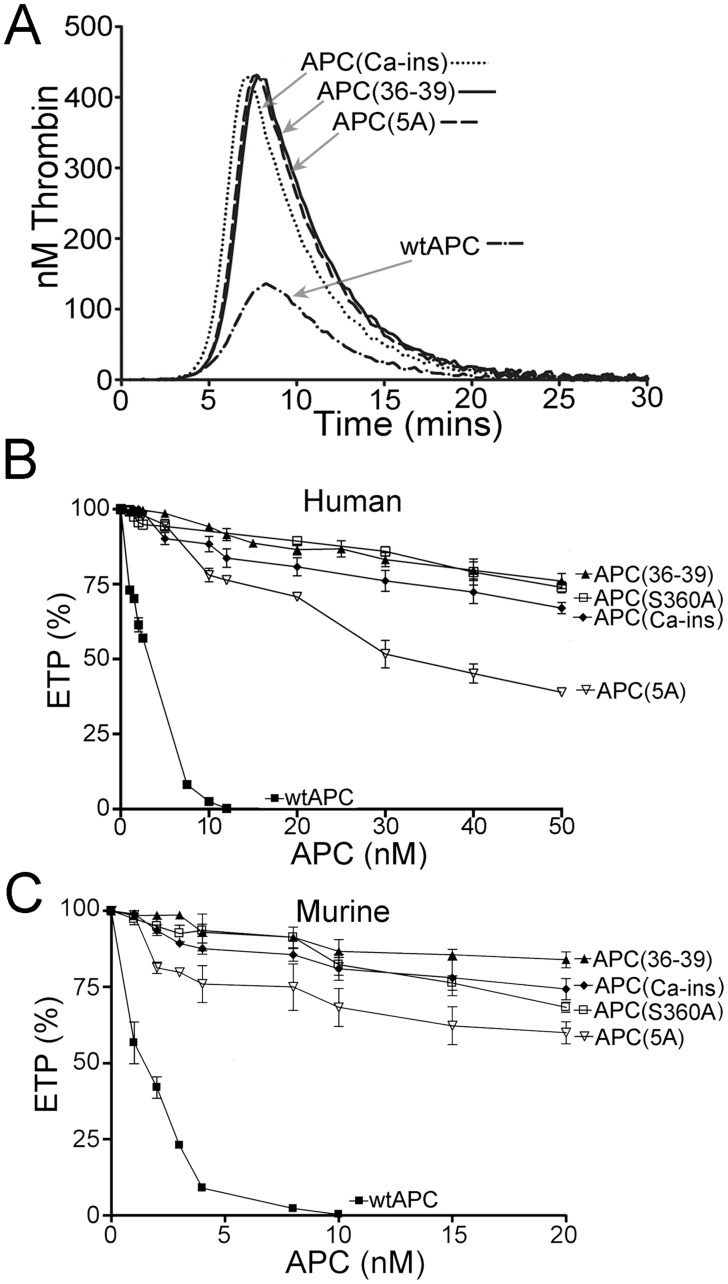
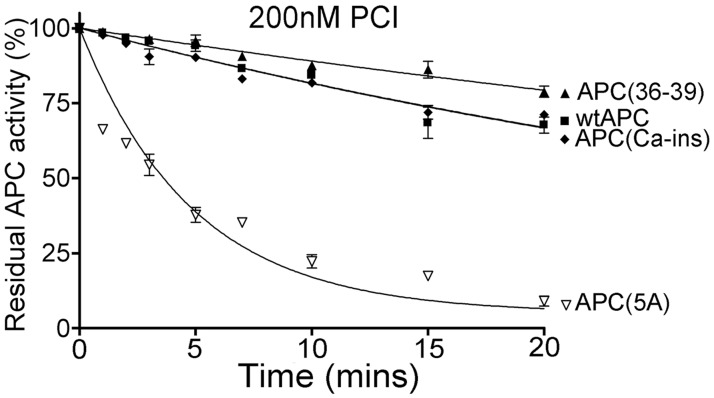
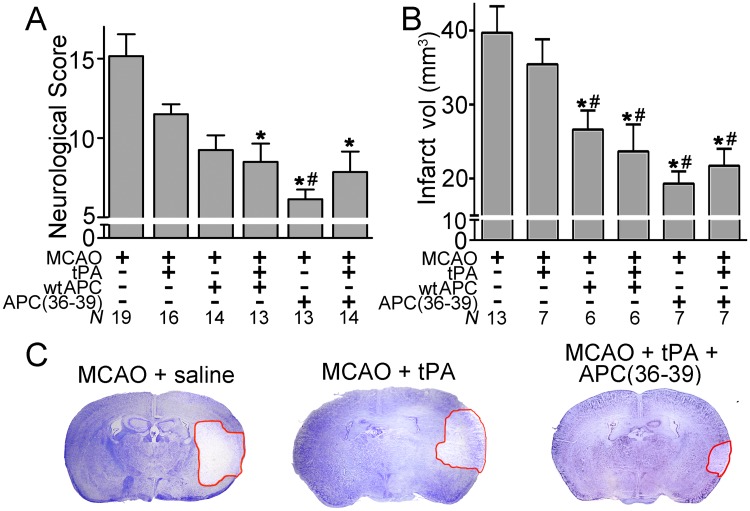
Ischaemic stroke is caused by occlusive thrombi in the cerebral vasculature. Although tissue-plasminogen activator (tPA) can be administered as thrombolytic therapy, it has major limitations, which include disruption of the blood-brain barrier and an increased risk of bleeding. Treatments that prevent or limit such deleterious effects could be of major clinical importance. Activated protein C (APC) is a natural anticoagulant that regulates thrombin generation, but also confers endothelial cytoprotective effects and improved endothelial barrier function mediated through its cell signalling properties. In murine models of stroke, although APC can limit the deleterious effects of tPA due to its cell signalling function, its anticoagulant actions can further elevate the risk of bleeding. Thus, APC variants such as APC(5A), APC(Ca-ins) and APC(36-39) with reduced anticoagulant, but normal signalling function may have therapeutic benefit. Human and murine protein C (5A), (Ca-ins) and (36-39) variants were expressed and characterised. All protein C variants were secreted normally, but 5-20% of the protein C (Ca-ins) variants were secreted as disulphide-linked dimers. Thrombin generation assays suggested reductions in anticoagulant function of 50- to 57-fold for APC(36-39), 22- to 27-fold for APC(Ca-ins) and 14- to 17-fold for APC(5A). Interestingly, whereas human wt APC, APC(36-39) and APC(Ca-ins) were inhibited similarly by protein C inhibitor (t½ - 33 to 39 mins), APC(5A) was inactivated ~9-fold faster (t½ - 4 mins). Using the murine middle cerebral artery occlusion ischaemia/repurfusion injury model, in combination with tPA, APC(36-39), which cannot be enhanced by its cofactor protein S, significantly improved neurological scores, reduced cerebral infarct area by ~50% and reduced oedema ratio. APC(36-39) also significantly reduced bleeding in the brain induced by administration of tPA, whereas wt APC did not. If our data can be extrapolated to clinical settings, then APC(36-39) could represent a feasible adjunctive therapy for ischaemic stroke.
缺血性中风是由脑血管中的闭塞性血栓引起的。尽管组织型纤溶酶原激活剂(tPA)可作为溶栓疗法使用,但其存在重大局限性,包括破坏血脑屏障以及出血风险增加。预防或限制此类有害影响的治疗方法可能具有重要的临床意义。活化蛋白C(APC)是一种天然抗凝剂,可调节凝血酶生成,还具有内皮细胞保护作用,并通过其细胞信号特性改善内皮屏障功能。在中风的小鼠模型中,尽管APC因其细胞信号功能可限制tPA的有害影响,但其抗凝作用会进一步增加出血风险。因此,抗凝功能降低但信号功能正常的APC变体,如APC(5A)、APC(Ca-ins)和APC(36-39)可能具有治疗益处。对人和小鼠的蛋白C(5A)、(Ca-ins)和(36-39)变体进行了表达和特性分析。所有蛋白C变体均正常分泌,但5%至20%的蛋白C(Ca-ins)变体以二硫键连接的二聚体形式分泌。凝血酶生成试验表明,APC(36-39)的抗凝功能降低了50至57倍,APC(Ca-ins)降低了22至27倍,APC(5A)降低了14至17倍。有趣的是,虽然人野生型APC、APC(36-39)和APC(Ca-ins)被蛋白C抑制剂抑制的情况相似(半衰期为33至39分钟),但APC(5A)的失活速度快约9倍(半衰期为4分钟)。使用小鼠大脑中动脉闭塞缺血/再灌注损伤模型,并联合tPA,不能被其辅因子蛋白S增强的APC(36-39)显著改善了神经功能评分,使脑梗死面积减少了约50%,并降低了水肿率。APC(36-39)还显著减少了tPA给药引起的脑出血,而野生型APC则没有。如果我们的数据能够外推至临床情况,那么APC(36-39)可能是缺血性中风一种可行的辅助治疗方法。