Lucero Emiliano, Collin Simon M, Gomes Sujit, Akter Fatima, Asad Asaduzzam, Kumar Das Asish, Ritmeijer Koert
Institute of Tropical Medicine and International Health, Charité-Universitätsmedizin Berlin, Germany; Centro de Estudios e Investigación de la Enfermedad de Chagas y Leishmaniasis-Universidad Nacional de Cordoba, Argentina.
School of Social & Community Medicine, University of Bristol, United Kingdom.
PLoS Negl Trop Dis. 2015 Apr 2;9(4):e0003699. doi: 10.1371/journal.pntd.0003699. eCollection 2015 Apr.
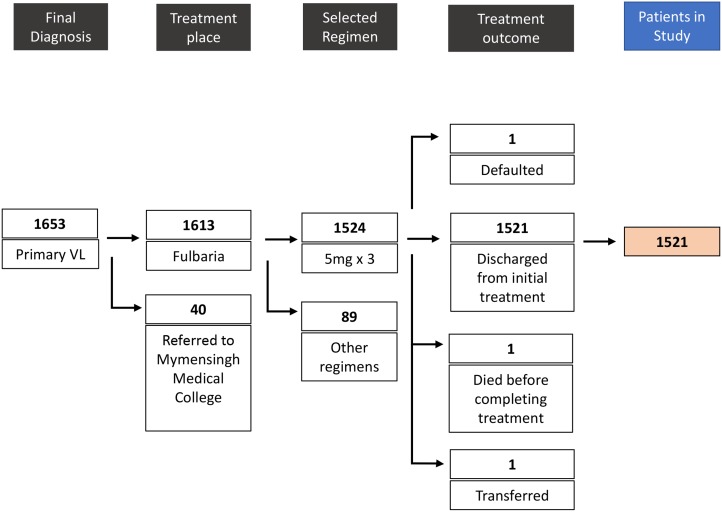
Bangladesh is one of the endemic countries for Visceral Leishmaniasis (VL). Médecins Sans Frontières (MSF) ran a VL treatment clinic in the most endemic district (Fulbaria) between 2010 and 2013 using a semi-ambulatory regimen for primary VL of 15 mg/kg Liposomal Amphotericin-B (AmBisome) in three equal doses of 5 mg/kg. The main objective of this study was to analyze the effectiveness and safety of this regimen after a 12 month follow-up period by retrospective analysis of routinely collected program data. A secondary objective was to explore risk factors for relapse.
Our analysis included 1521 patients who were initially cured, of whom 1278 (84%) and 1179 (77.5%) were followed-up at 6 and 12 months, respectively. Cure rates at 6 and 12 months were 98.7% (1262/1278) and 96.4% (1137/1179), respectively. Most relapses (26/39) occurred between 6 and 12 months after treatment. Serious adverse events (SAE) were recorded for 7 patients (0.5%). Odds of relapse at 12 months were highest in the youngest and oldest age groups. There was some evidence that spleen size measured on discharge (one month after initiation of treatment) was associated with risk of relapse: OR=1.25 (95% CI 1.01 to 1.55) per cm below lower costal margin (P=0.04).
Our study demonstrates that 15 mg/kg AmBisome in three doses of 5 mg/kg is an effective (>95% cure rate) and safe (<1% SAE) treatment for primary VL in Bangladesh. The majority of relapses occurred between 6 and 12 months, justifying the use of a longer follow-up period when feasible. Assessment of risk of relapse based on easily measured clinical parameters such as spleen size could be incorporated in VL treatment protocols in resource-poor settings where test-of-cure is not always feasible.
孟加拉国是内脏利什曼病(VL)的流行国家之一。无国界医生组织(MSF)于2010年至2013年期间在流行程度最高的地区(富尔巴里)开办了一家VL治疗诊所,采用半门诊治疗方案,即使用15毫克/千克脂质体两性霉素B(安必素),分三次等量给予,每次5毫克/千克,用于初治VL。本研究的主要目的是通过对常规收集的项目数据进行回顾性分析,在12个月的随访期后分析该方案的有效性和安全性。次要目的是探讨复发的危险因素。
我们的分析纳入了1521例最初治愈的患者,其中分别有1278例(84%)和1179例(77.5%)在6个月和12个月时接受了随访。6个月和12个月时的治愈率分别为98.7%(1262/1278)和96.4%(1137/1179)。大多数复发(26/39)发生在治疗后6至12个月之间。记录到7例患者(0.5%)出现严重不良事件(SAE)。12个月时复发的几率在最年轻和最年长的年龄组中最高。有证据表明,出院时(治疗开始后1个月)测量的脾脏大小与复发风险相关:低于肋下缘每厘米的比值比(OR)为1.25(95%置信区间1.01至1.55)(P = 0.04)。
我们的研究表明,15毫克/千克安必素分三次每次5毫克/千克的剂量是孟加拉国初治VL的一种有效(治愈率>95%)且安全(SAE<1%)的治疗方法。大多数复发发生在6至12个月之间,这证明在可行的情况下使用更长的随访期是合理 的。在资源匮乏地区,当治愈检测并不总是可行时,基于脾脏大小等易于测量的临床参数评估复发风险可纳入VL治疗方案。