Cefalu William T, Leiter Lawrence A, de Bruin Tjerk W A, Gause-Nilsson Ingrid, Sugg Jennifer, Parikh Shamik J
Pennington Biomedical Research Center, Louisiana State University, Baton Rouge, LA
Keenan Research Center in the Li Ka Shing Knowledge Institute, St. Michael's Hospital, and Division of Endocrinology & Metabolism, University of Toronto, Toronto, Canada.
Diabetes Care. 2015 Jul;38(7):1218-27. doi: 10.2337/dc14-0315. Epub 2015 Apr 7.
To assess the efficacy and safety of dapagliflozin, a selective sodium-glucose cotransporter 2 inhibitor, compared with placebo in patients with type 2 diabetes (T2D), documented pre-existing cardiovascular disease (CVD), and a history of hypertension.
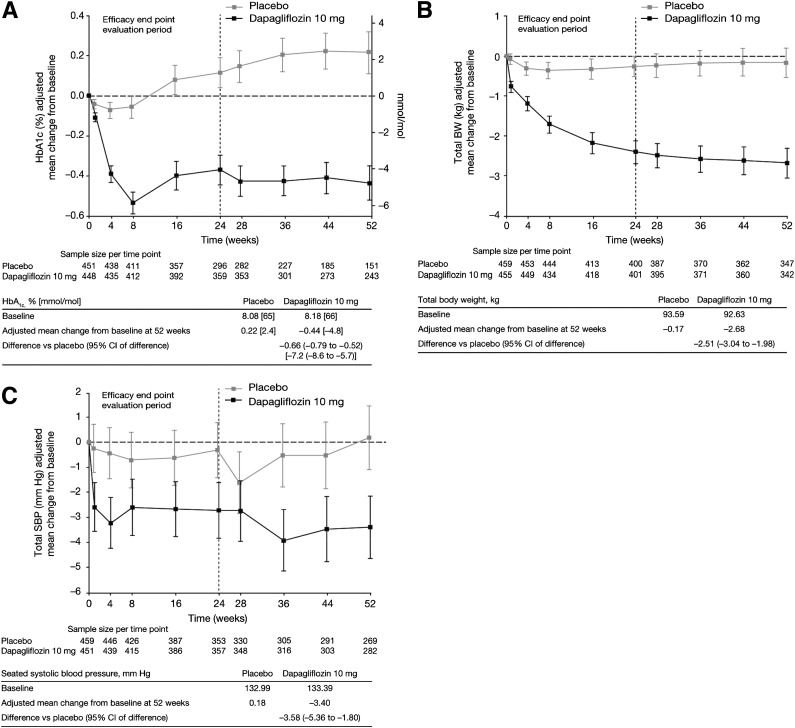
Patients (N = 922) were randomized to receive 10 mg dapagliflozin or placebo in a double-blind trial for 24 weeks, followed by a 28-week extension period. In patients receiving insulin, the insulin dose was reduced by 25% at randomization. Patients were stratified by age, insulin use, and time from the most recent qualifying cardiovascular (CV) event. Co-primary end points were a change from baseline in hemoglobin A1c (HbA1c) and the proportion of patients achieving a combined reduction in HbA1c of ≥0.5% (5.5 mmol/mol), body weight (BW) of ≥3%, and systolic blood pressure (SBP) of ≥3 mmHg.
At 24 weeks, dapagliflozin significantly reduced HbA1c (-0.38% [-4.2 mmol/mol]) from baseline (8.18%) compared with a slight increase with placebo from baseline (8.08%) (0.08% [0.9 mmol/mol]). Significantly more patients met the three-item end point with treatment with dapagliflozin than with placebo (11.7% vs. 0.9%, respectively). Changes were maintained over 52 weeks. Although ∼42% of patients were ≥65 years old, similar results were observed in both age-stratified groups. Serious adverse events, hypoglycemia, urinary tract infections, and cardiac disorders were similar between groups. Adverse events of hypotension, dehydration, hypovolemia, genital infection, and renal failure or impairment occurred more often with dapagliflozin treatment.
In this study that evaluated T2D patients who were at high risk for future CVD events, dapagliflozin administration had significantly greater effects in reducing HbA1c, BW, and SBP, without adversely impacting CV safety when compared with placebo treatment.
评估选择性钠-葡萄糖协同转运蛋白2抑制剂达格列净与安慰剂相比,在2型糖尿病(T2D)、已确诊的心血管疾病(CVD)和高血压病史患者中的疗效和安全性。
在一项双盲试验中,将922例患者随机分为接受10 mg达格列净或安慰剂治疗24周,随后为28周的延长期。接受胰岛素治疗的患者,在随机分组时胰岛素剂量降低25%。患者按年龄、胰岛素使用情况以及距最近一次符合条件的心血管(CV)事件的时间进行分层。共同主要终点为糖化血红蛋白(HbA1c)较基线的变化,以及HbA1c联合降低≥0.5%(5.5 mmol/mol)、体重(BW)降低≥3%和收缩压(SBP)降低≥3 mmHg的患者比例。
在24周时,与安慰剂组基线(8.08%)轻微升高(0.08% [0.9 mmol/mol])相比,达格列净组HbA1c较基线(8.18%)显著降低(-0.38% [-4.2 mmol/mol])。与安慰剂组相比,接受达格列净治疗达到三项终点的患者显著更多(分别为11.7%和0.9%)。这些变化在52周内得以维持。尽管约42%的患者年龄≥65岁,但在两个年龄分层组中均观察到类似结果。两组间严重不良事件、低血糖、尿路感染和心脏疾病相似。达格列净治疗时,低血压、脱水、血容量不足、生殖器感染以及肾衰竭或损害等不良事件更常发生。
在这项评估未来发生CVD事件高危的T2D患者的研究中,与安慰剂治疗相比,使用达格列净在降低HbA1c、BW和SBP方面有显著更大的效果,且未对心血管安全性产生不利影响。