Baldan V, Griffiths R, Hawkins R E, Gilham D E
Clinical and Experimental Immunotherapy Group, Institute of Cancer Sciences, University of Manchester, Manchester Academic Healthcare Science Centre, Paterson Building, Withington, Manchester M20 4BX, UK.
1] Clinical and Experimental Immunotherapy Group, Institute of Cancer Sciences, University of Manchester, Manchester Academic Healthcare Science Centre, Paterson Building, Withington, Manchester M20 4BX, UK [2] The Clatterbridge Cancer Centre, Clatterbridge Road, Wirral CH63 4JY, UK.
Br J Cancer. 2015 Apr 28;112(9):1510-8. doi: 10.1038/bjc.2015.96. Epub 2015 Mar 17.
Tumour-infiltrating lymphocyte (TIL) therapy is showing great promise in the treatment of patients with advanced malignant melanoma. However, the translation of TIL therapy to non-melanoma tumours such as renal cell carcinoma has been less successful with a major constraint being the inability to reproducibly generate TILs from primary and metastatic tumour tissue.
Primary and metastatic renal cell carcinoma biopsies were subjected to differential tumour disaggregation methods and procedures that stimulate the specific expansion of TILs tested to determine which reliably generated TIL maintained antitumour specificity.
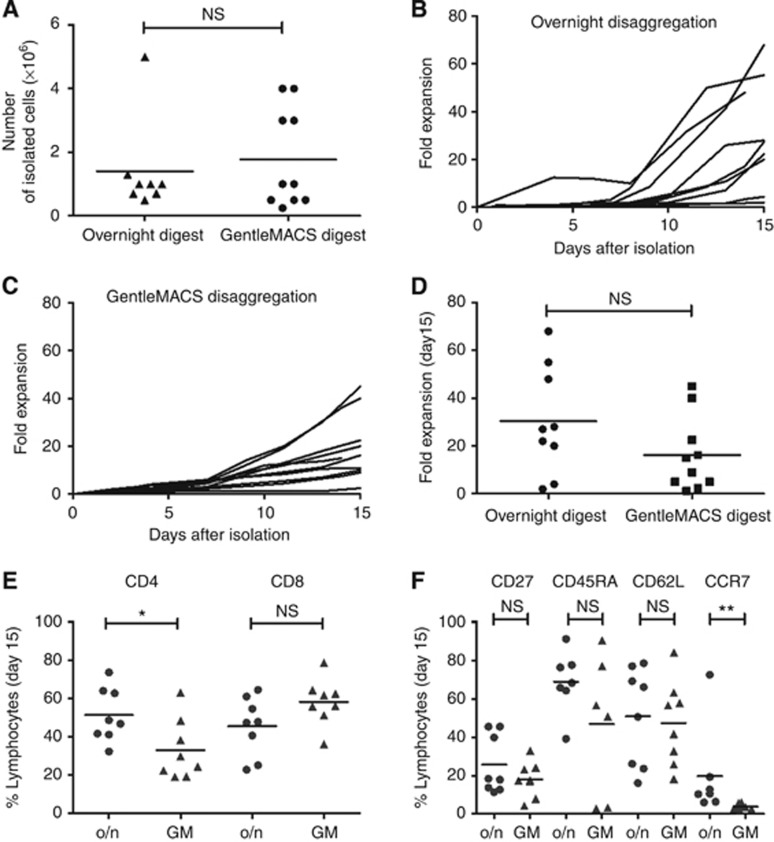
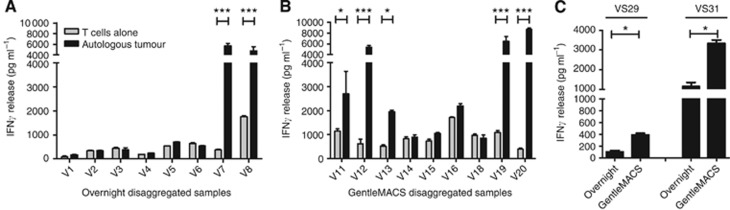
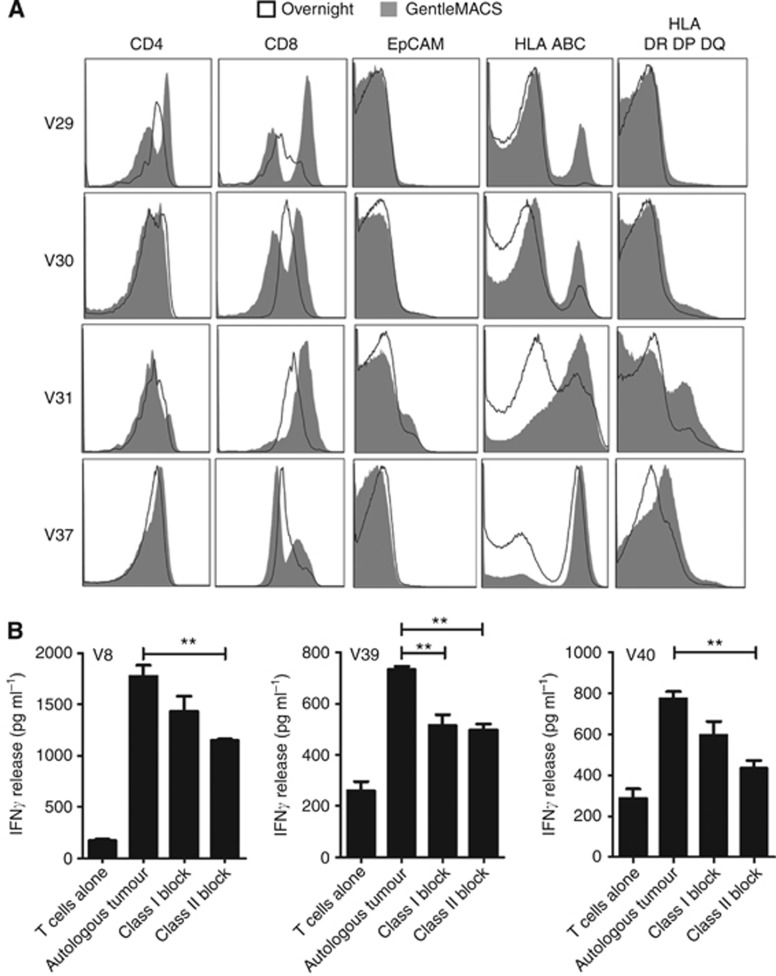
Enzymatic or combined enzymatic/mechanical disaggregation resulted in equivalent numbers of TILs being liberated from renal cell carcinoma biopsies. Following mitogenic activation of the isolated TILs with anti-CD3/anti-CD28-coated paramagnetic beads, successful TIL expansion was achieved in 90% of initiated cultures. The frequency of T-cell recognition of autologous tumours was enhanced when tumours were disaggregated using the GentleMACS enzymatic/mechanical system.
TILs can be consistently produced from renal cell carcinoma biopsies maintaining autologous tumour recognition after expansion in vitro. While the method of disaggregation has little impact on the success of TIL growth, methods that preserve the cell surface architecture facilitate TIL recognition of an autologous tumour, which is important in terms of characterising the functionality of the expanded TIL population.
肿瘤浸润淋巴细胞(TIL)疗法在晚期恶性黑色素瘤患者的治疗中显示出巨大潜力。然而,将TIL疗法应用于肾细胞癌等非黑色素瘤肿瘤的效果不太理想,主要限制在于无法从原发性和转移性肿瘤组织中可重复地产生TIL。
对原发性和转移性肾细胞癌活检组织采用不同的肿瘤解离方法和刺激TIL特异性扩增的程序进行测试,以确定哪种方法能可靠地产生保持抗肿瘤特异性的TIL。
酶解或酶解/机械联合解离从肾细胞癌活检组织中释放出的TIL数量相当。用抗CD3/抗CD28包被的顺磁性微珠对分离出的TIL进行促有丝分裂激活后,90%的起始培养物成功实现了TIL扩增。当使用GentleMACS酶解/机械系统解离肿瘤时,T细胞对自体肿瘤的识别频率增加。
肾细胞癌活检组织能够持续产生TIL,体外扩增后仍保持对自体肿瘤的识别能力。虽然解离方法对TIL生长的成功率影响不大,但保留细胞表面结构的方法有助于TIL识别自体肿瘤,这对于表征扩增的TIL群体的功能很重要。