Duong Vu H, Baer Maria R, Hendrick Franklin, Weiss Sheila R, Sato Masayo, Zeidan Amer M, Gore Steven D, Davidoff Amy J
University of Maryland Marlene and Stewart Greenebaum Cancer Center and Department of Medicine, University of Maryland School of Medicine, Baltimore, MD, USA.
University of Maryland Marlene and Stewart Greenebaum Cancer Center and Department of Medicine, University of Maryland School of Medicine, Baltimore, MD, USA.
Leuk Res. 2015 Jun;39(6):586-91. doi: 10.1016/j.leukres.2015.03.013. Epub 2015 Mar 28.
Erythropoiesis-stimulating agents (ESAs) reduce red blood cell (RBC) transfusions in approximately 40% of patients with myelodysplastic syndrome (MDS) in clinical trials. We studied the association of timing of ESA initiation, agent (epoetin alfa, darbepoetin) and number of weeks of ESA use with response in MDS patients in routine practice.
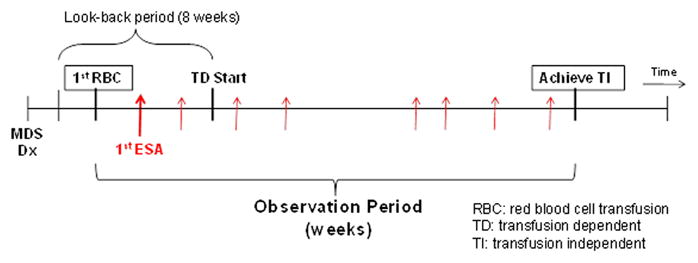
Patients diagnosed with MDS from 2001 to 2005 were identified in the Surveillance Epidemiology and End Results-Medicare linked database. The study cohort consisted of patients with new-onset transfusion dependence (TD). All patients received an ESA at least once during the study period, which began the week that criteria for TD were met and continued until transfusion independence (TI). Kaplan-Meier statistics and Cox Proportional Hazard models were used to assess relationships between time to ESA initiation, agent and number of weeks of ESA use and TI attainment.
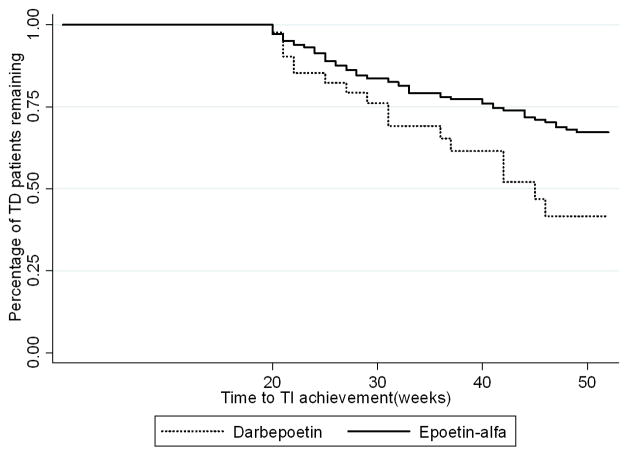
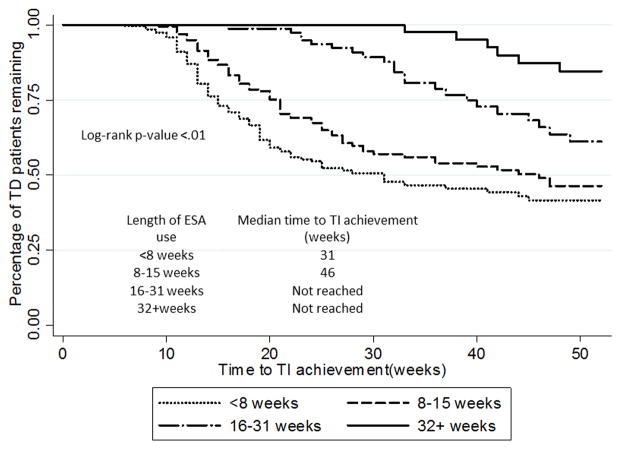
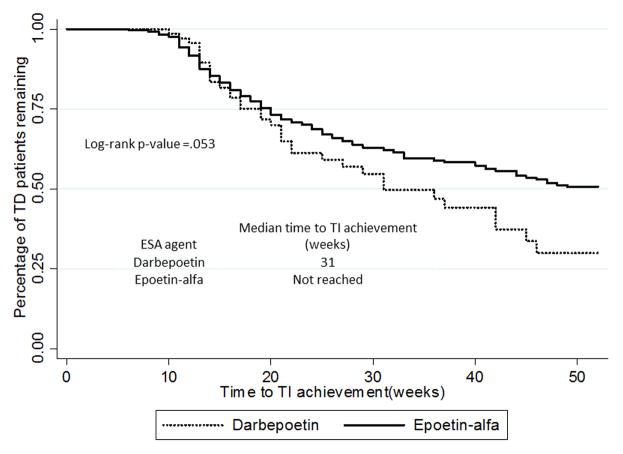
Of 610 TD patients treated with ESAs, 210 (34.4%) achieved TI. Median time from ESA initiation to TI was 13 weeks. Shorter time from TD to ESA initiation and use of darbepoetin were associated with higher probability of achieving TI. The probability of achieving TI decreased beyond 8 weeks of treatment, and was very low beyond 16 weeks (8-15 weeks: HR=0.64, 16-31 weeks: HR=0.25, 32+ weeks HR=0.10).
In this observational, population-based study, variations in ESA administration impacted response in transfusion-dependent MDS patients, with higher response rates with early administration and use of darbepoetin, and low response likelihood in non-responders beyond 16 weeks of therapy.
在临床试验中,促红细胞生成素(ESAs)可使约40%的骨髓增生异常综合征(MDS)患者减少红细胞(RBC)输血。我们在常规实践中研究了MDS患者开始使用ESA的时间、药物(促红细胞生成素α、达比泊汀)以及使用ESA的周数与反应之间的关联。
在监测、流行病学和最终结果-医疗保险链接数据库中识别出2001年至2005年诊断为MDS的患者。研究队列包括新发性输血依赖(TD)患者。所有患者在研究期间至少接受过一次ESA治疗,研究从满足TD标准的那一周开始,持续至输血独立(TI)。使用Kaplan-Meier统计和Cox比例风险模型评估开始使用ESA的时间、药物以及使用ESA的周数与实现TI之间的关系。
在610例接受ESA治疗的TD患者中,210例(34.4%)实现了TI。从开始使用ESA到TI的中位时间为13周。从TD到开始使用ESA的时间较短以及使用达比泊汀与实现TI的较高概率相关。治疗超过8周后实现TI的概率降低,超过16周时非常低(8 - 15周:风险比[HR]=0.64,16 - 31周:HR=0.25,32周及以上:HR=0.10)。
在这项基于人群的观察性研究中,ESA给药的差异影响了输血依赖型MDS患者的反应,早期给药和使用达比泊汀的反应率较高,治疗16周后无反应者的反应可能性较低。