Ahmed L A, Shigdel R, Joakimsen R M, Eldevik O P, Eriksen E F, Ghasem-Zadeh A, Bala Y, Zebaze R, Seeman E, Bjørnerem Å
Department of Health and Care Sciences, UiT-The Arctic University of Norway, Tromsø, Norway.
Osteoporos Int. 2015 Aug;26(8):2137-46. doi: 10.1007/s00198-015-3118-x. Epub 2015 Apr 16.
We tested whether cortical porosity of the proximal femur measured using StrAx1.0 software provides additional information to areal bone mineral density (aBMD) or Fracture Risk Assessment Tool (FRAX) in differentiating women with and without fracture. Porosity was associated with fracture independent of aBMD and FRAX and identified additional women with fractures than by osteoporosis or FRAX thresholds.
Neither aBMD nor the FRAX captures cortical porosity, a major determinant of bone strength. We therefore tested whether combining porosity with aBMD or FRAX improves identification of women with fractures.
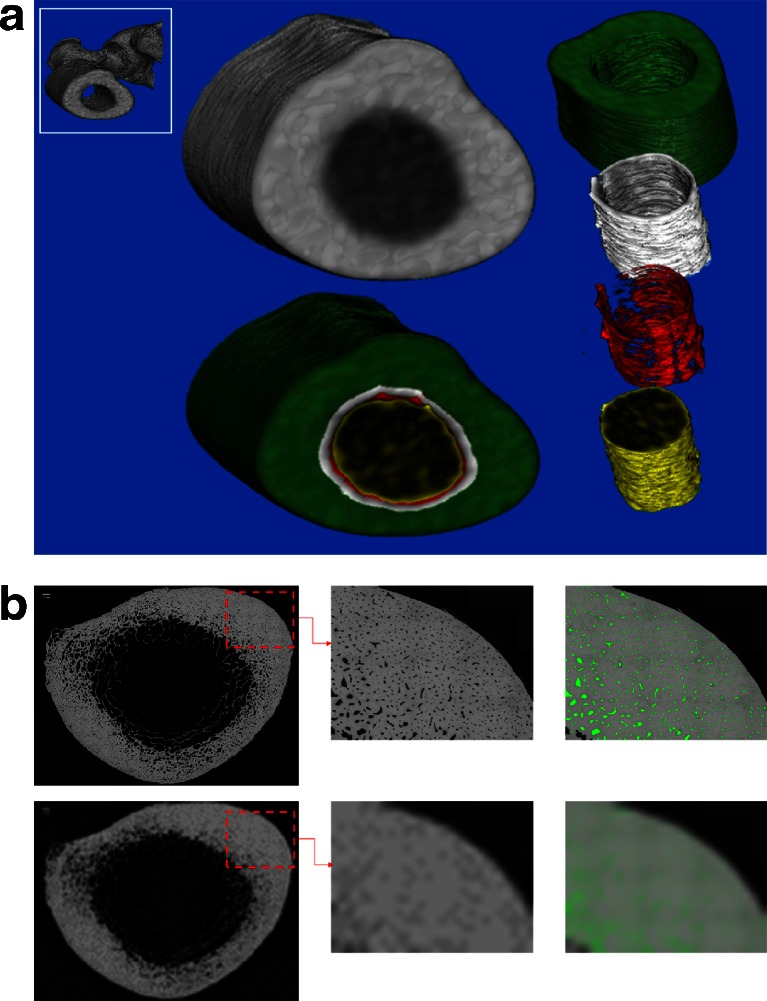
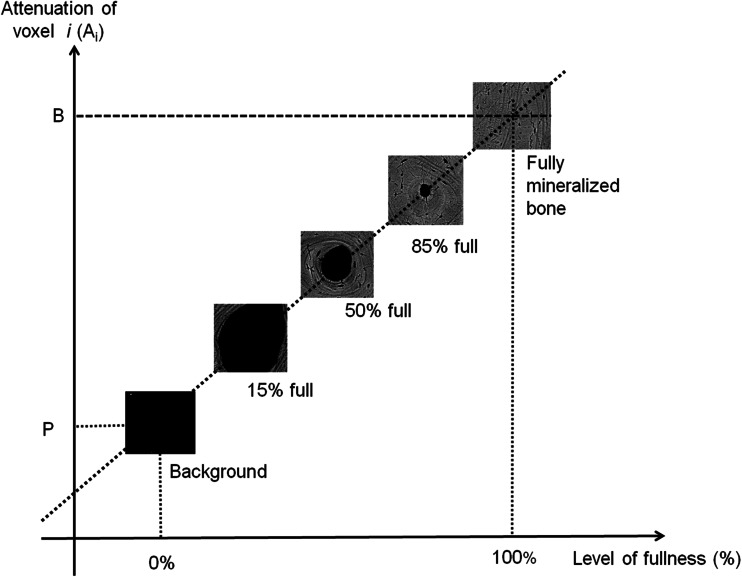
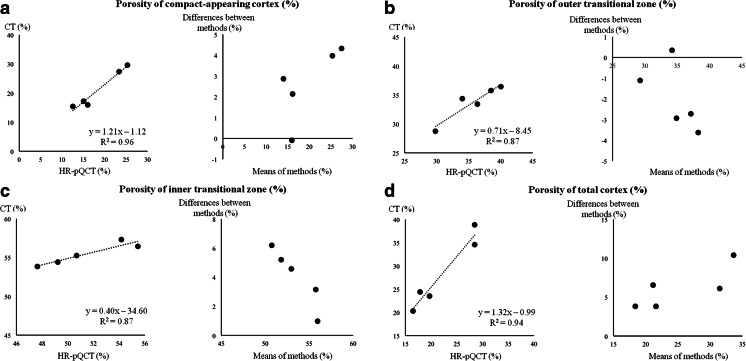
We quantified femoral neck (FN) aBMD using dual-energy X-ray absorptiometry, FRAX score, and femoral subtrochanteric cortical porosity using StrAx1.0 software in 211 postmenopausal women aged 54-94 years with nonvertebral fractures and 232 controls in Tromsø, Norway. Odds ratios (ORs) were calculated using logistic regression analysis.
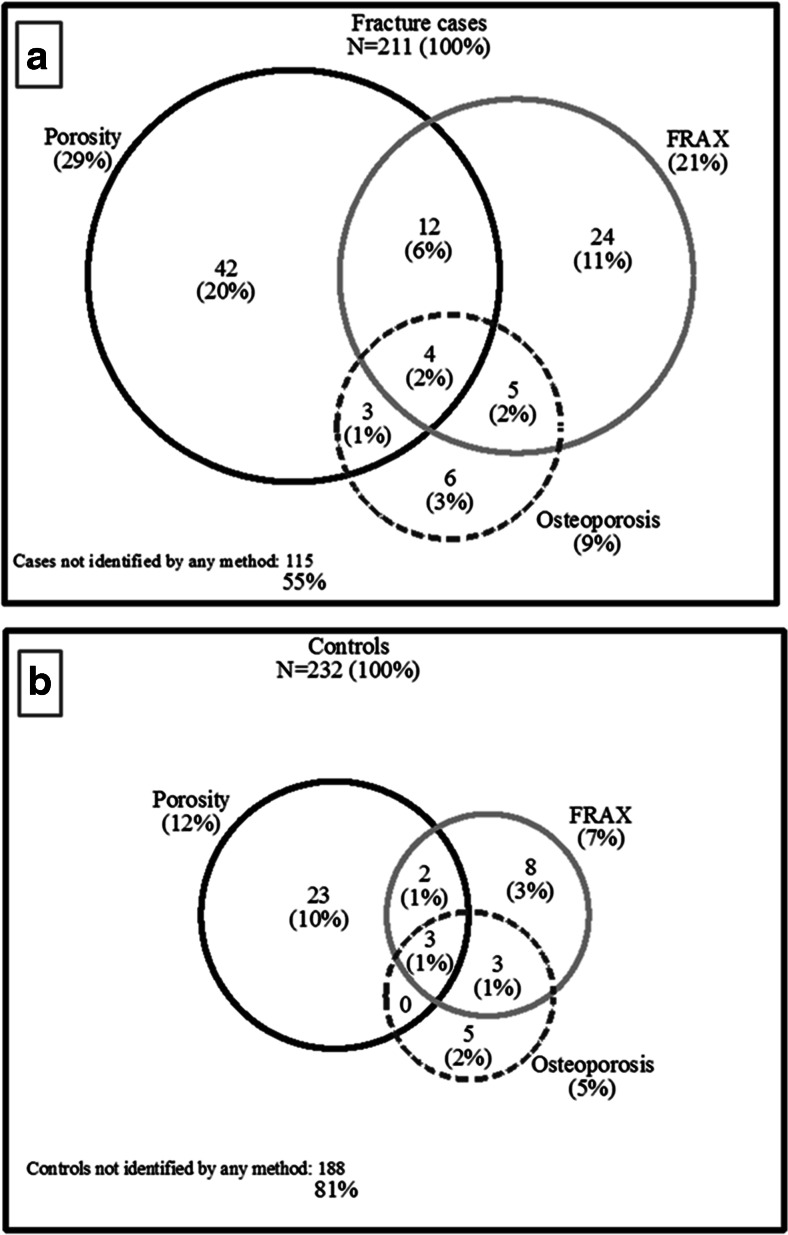
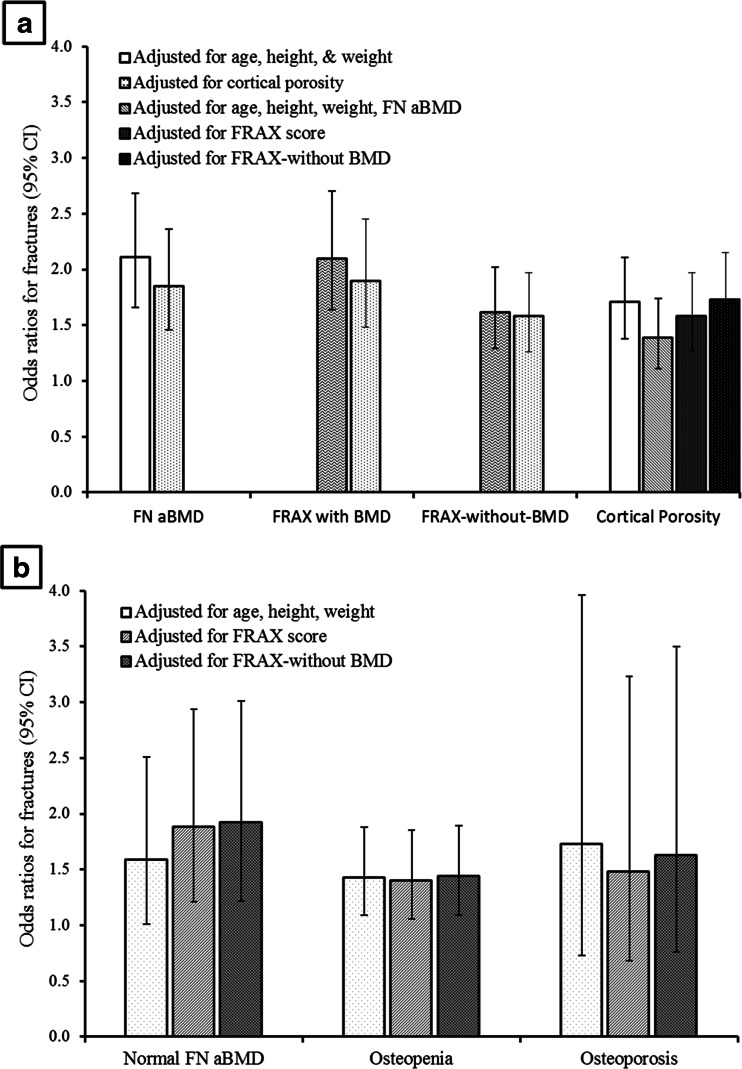
Women with fractures had lower FN aBMD, higher FRAX score, and higher cortical porosity than controls (all p < 0.001). Each standard deviation higher porosity was associated with fracture independent of FN aBMD (OR 1.39; 95% confidence interval 1.11-1.74) and FRAX score (OR 1.58; 1.27-1.97) in all women combined. Porosity was also associated with fracture independent of FRAX score in subgroups with normal FN aBMD (OR 1.88; 1.21-2.94), osteopenia (OR 1.40; 1.06-1.85), but not significantly in those with osteoporosis (OR 1.48; 0.68-3.23). Of the 211 fracture cases, only 18 women (9%) were identified using FN aBMD T-score < -2.5, 45 women (21%) using FRAX threshold >20%, whereas porosity >80th percentile identified 61 women (29%). Porosity identified 26% additional women with fractures than identified by the osteoporosis threshold and 21% additional women with fractures than by this FRAX threshold.
Cortical porosity is a risk factor for fracture independent of aBMD and FRAX and improves identification of women with fracture.
我们测试了使用StrAx1.0软件测量的股骨近端皮质孔隙率,在区分有骨折和无骨折的女性时,是否能为骨面积密度(aBMD)或骨折风险评估工具(FRAX)提供额外信息。孔隙率与骨折相关,独立于aBMD和FRAX,并且比通过骨质疏松症或FRAX阈值识别出更多有骨折的女性。
aBMD和FRAX都未考虑皮质孔隙率,而皮质孔隙率是骨强度的主要决定因素。因此,我们测试了将孔隙率与aBMD或FRAX相结合,是否能更好地识别有骨折的女性。
我们使用双能X线吸收法对211名年龄在54 - 94岁、有非椎体骨折的绝经后挪威特罗姆瑟女性和232名对照者的股骨颈(FN)aBMD、FRAX评分进行了量化,并使用StrAx1.0软件对股骨转子下皮质孔隙率进行了量化。使用逻辑回归分析计算比值比(OR)。
与对照组相比,有骨折的女性FN aBMD更低、FRAX评分更高、皮质孔隙率更高(所有p < 0.001)。在所有女性中,孔隙率每增加一个标准差,独立于FN aBMD(OR 1.39;95%置信区间1.11 - 1.74)和FRAX评分(OR 1.58;1.27 - 1.97)与骨折相关。在FN aBMD正常的亚组(OR 1.88;1.21 - 2.94)、骨质减少亚组(OR 1.40;1.06 - 1.85)中,孔隙率也独立于FRAX评分与骨折相关,但在骨质疏松症亚组中无显著相关性(OR 1.48;0.68 - 3.23)。在211例骨折病例中,仅18名女性(9%)通过FN aBMD T评分< -2.5被识别,45名女性(21%)通过FRAX阈值>20%被识别,而孔隙率>第80百分位数识别出61名女性(29%)。与骨质疏松症阈值相比,孔隙率识别出多26%有骨折的女性;与该FRAX阈值相比,孔隙率识别出多21%有骨折的女性。
皮质孔隙率是独立于aBMD和FRAX的骨折危险因素,能更好地识别有骨折的女性。