Dhoro Milcah, Zvada Simbarashe, Ngara Bernard, Nhachi Charles, Kadzirange Gerald, Chonzi Prosper, Masimirembwa Collen
Department of Molecular Sciences, African Institute of Biomedical Science and Technology, Dominion House, 211 Herbert Chitepo Street, P.O. Box 2294, Harare, Zimbabwe.
Department of Clinical Pharmacology, College of Health Sciences, University of Zimbabwe, Harare, Zimbabwe.
BMC Pharmacol Toxicol. 2015 Mar 27;16:4. doi: 10.1186/s40360-015-0004-2.
Efavirenz (EFV) therapeutic response and toxicity are associated with high inter-individual variability attributed to variation in its pharmacokinetics. Plasma concentrations below 1 μg/ml may result in virologic failure and above 4 μg/ml, may result in central nervous system adverse effects. This study used population pharmacokinetics modeling to explore the influence of demographic and pharmacogenetic factors including efavirenz-rifampicin interaction on EFV pharmacokinetics, towards safer dosing of EFV.
Patients receiving an EFV-based regimen for their antiretroviral therapy and a rifampicin-containing anti-TB regimen were recruited. EFV plasma concentrations were measured by HPLC and genomic DNA genotyped for variants in the CYP2B6, CYP2A6 and ABCB1 genes. All patients were evaluated for central nervous system adverse effects characterised as sleep disorders, hallucinations and headaches using the WHO ADR grading system. A pharmacokinetic model was built in a forward and reverse procedure using nonlinear mixed effect modeling in NONMEM VI followed by model-based simulations for optimal doses.
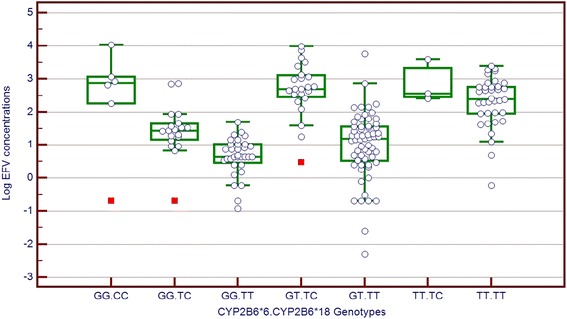
CYP2B66 and 18 variant alleles, weight and sex were the most significant covariates explaining 55% of inter-individual variability in EFV clearance. Patients with the CYP2B66TT genotype had a 63% decrease in EFV clearance despite their CYP2B618 genotypes with females having 22% higher clearance compared to males. There was a 21% increase in clearance for every 10 kg increase in weight. The effect of TB/HIV co-treatment versus HIV treatment only was not statistically significant. No clinically relevant association between CYP2B6 genotypes and CNS adverse effects was seen, but patients with CNS adverse effects had a 27% lower clearance compared to those without. Model- based simulations indicated that all carriers of CYP2B6*6 TT genotype would be recommended a dose reduction to 200 mg/day, while the majority of extensive metabolisers may be given 400 mg/day and still maintain therapeutic levels.
This study showed that screening for CYP2B6 functional variants has a high predictability for efavirenz plasma levels and could be used in prescribing optimal and safe EFV doses.
依非韦伦(EFV)的治疗反应和毒性存在较高的个体间差异,这归因于其药代动力学的变化。血浆浓度低于1μg/ml可能导致病毒学治疗失败,而高于4μg/ml可能导致中枢神经系统不良反应。本研究采用群体药代动力学建模来探讨人口统计学和药物遗传学因素(包括依非韦伦-利福平相互作用)对EFV药代动力学的影响,以实现更安全的EFV给药。
招募接受基于EFV的抗逆转录病毒治疗方案以及含利福平的抗结核治疗方案的患者。通过高效液相色谱法测定EFV血浆浓度,并对CYP2B6、CYP2A6和ABCB1基因的变体进行基因组DNA基因分型。使用世界卫生组织药物不良反应分级系统对所有患者的中枢神经系统不良反应进行评估,这些不良反应表现为睡眠障碍、幻觉和头痛。使用NONMEM VI中的非线性混合效应建模,通过正向和反向程序建立药代动力学模型,随后进行基于模型的模拟以确定最佳剂量。
CYP2B66和18变异等位基因、体重和性别是解释EFV清除率个体间差异55%的最显著协变量。CYP2B66TT基因型的患者,无论其CYP2B618基因型如何,EFV清除率均降低63%,女性的清除率比男性高22%。体重每增加10kg,清除率增加21%。结核病/艾滋病联合治疗与单纯艾滋病治疗的效果无统计学显著差异。未观察到CYP2B6基因型与中枢神经系统不良反应之间存在临床相关关联,但有中枢神经系统不良反应的患者的清除率比无不良反应的患者低27%。基于模型的模拟表明,所有CYP2B6*6 TT基因型携带者建议将剂量减至200mg/天,而大多数广泛代谢者可给予400mg/天且仍能维持治疗水平。
本研究表明,筛查CYP2B6功能变体对依非韦伦血浆水平具有较高的预测性,可用于开具最佳和安全的EFV剂量。