Halfon Patricia, Eggli Yves, Morel Yves, Taffé Patrick
Institute of Social and Preventive Medicine (IUMSP), University Hospital Center and Faculty of Biology and Medicine, Biopole 2, Route de la Corniche 10, 1010, Lausanne, Switzerland.
Institute of Health Economics and Management, University Hospital Center and University of Lausanne, Route de Chavannes 31, 1015, Lausanne, Switzerland.
BMC Health Serv Res. 2015 Feb 7;15:52. doi: 10.1186/s12913-015-0686-6.
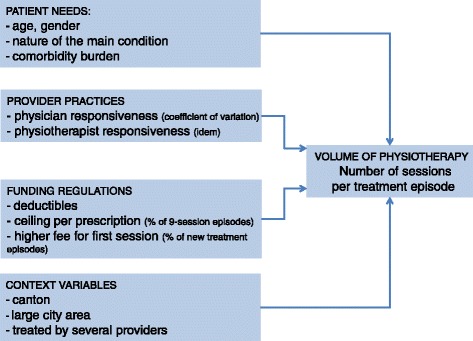
Many studies have found considerable variations in the resource intensity of physical therapy episodes. Although they have identified several patient- and provider-related factors, few studies have examined their relative explanatory power. We sought to quantify the contribution of patients and providers to these differences and examine how effective Swiss regulations are (nine-session ceiling per prescription and bonus for first treatments).
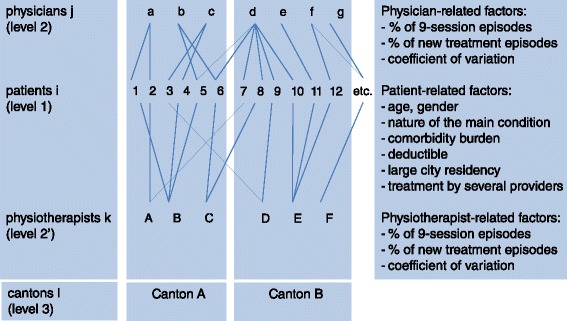
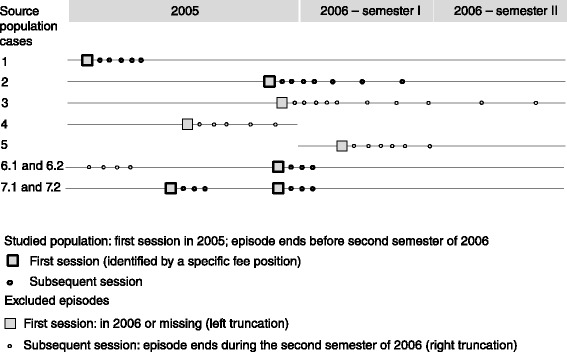
Our sample consisted of 87,866 first physical therapy episodes performed by 3,365 physiotherapists based on referrals by 6,131 physicians. We modeled the number of visits per episode using a multilevel log linear regression with crossed random effects for physiotherapists and physicians and with fixed effects for cantons. The three-level explanatory variables were patient, physiotherapist and physician characteristics.
The median number of sessions was nine (interquartile range 6-13). Physical therapy use increased with age, women, higher health care costs, lower deductibles, surgery and specific conditions. Use rose with the share of nine-session episodes among physiotherapists or physicians, but fell with the share of new treatments. Geographical area had no influence. Most of the variance was explained at the patient level, but the available factors explained only 4% thereof. Physiotherapists and physicians explained only 6% and 5% respectively of the variance, although the available factors explained most of this variance. Regulations were the most powerful factors.
Against the backdrop of abundant physical therapy supply, Swiss financial regulations did not restrict utilization. Given that patient-related factors explained most of the variance, this group should be subject to closer scrutiny. Moreover, further research is needed on the determinants of patient demand.
许多研究发现物理治疗疗程的资源强度存在显著差异。尽管他们已经确定了一些与患者和提供者相关的因素,但很少有研究考察它们的相对解释力。我们试图量化患者和提供者对这些差异的贡献,并研究瑞士的法规(每张处方九次治疗上限和首次治疗奖金)的有效性。
我们的样本包括由3365名物理治疗师根据6131名医生的转诊进行的87866次首次物理治疗疗程。我们使用多水平对数线性回归对每个疗程的就诊次数进行建模,对物理治疗师和医生采用交叉随机效应,对各州采用固定效应。三级解释变量为患者、物理治疗师和医生的特征。
疗程的中位数为9次(四分位间距为6 - 13次)。物理治疗的使用随着年龄、女性、更高的医疗费用、更低的免赔额、手术和特定疾病而增加。使用量随着物理治疗师或医生中九次治疗疗程的比例上升而上升,但随着新治疗的比例下降而下降。地理区域没有影响。大部分方差在患者层面得到解释,但可用因素仅解释了其中的4%。物理治疗师和医生分别仅解释了方差的6%和5%,尽管可用因素解释了大部分这种方差。法规是最有力的因素。
在物理治疗供应充足的背景下,瑞士的财务法规并未限制使用。鉴于与患者相关的因素解释了大部分方差,该群体应受到更密切的审查。此外,需要对患者需求的决定因素进行进一步研究。