Hayashi Shinya, Fujishiro Takaaki, Hashimoto Shingo, Kanzaki Noriyuki, Kuroda Ryosuke, Kurosaka Masahiro
Department of Orthopaedic Surgery, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-cho, Chuo-ku, Kobe, 650-0017, Japan.
J Orthop Surg Res. 2015 Apr 21;10:52. doi: 10.1186/s13018-015-0192-x.
Minimally invasive surgical approaches are widely used for total hip arthroplasty (THA). However, potential problems related to a reduced visual field during surgery, such as implant malposition, neurovascular injury, and poor implant fixation, have been reported. In these situations, a shorter stem is easier to insert in the femoral canal. To evaluate the accuracy of shorter stem orientation, we focused on the accuracy of stem orientation especially in short tapered wedge stems and evaluated the contribution factors of stem malalignment during mini-invasive total hip arthroplasty.
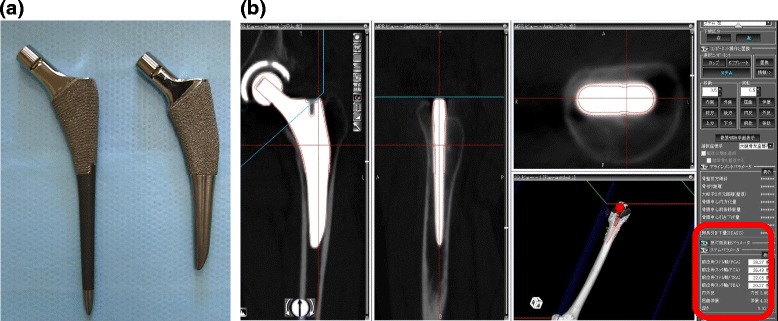
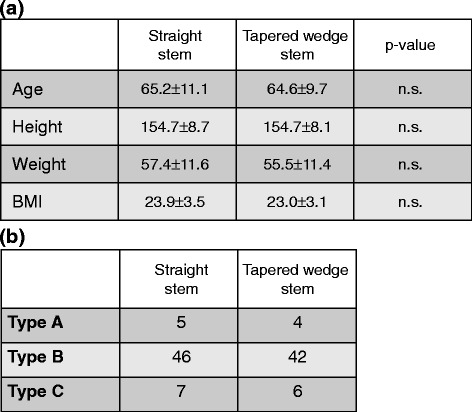
One hundred ten hips that underwent THA with a Summit stem (58 hips) (DePuy, Warsaw, IN) as straight stem and TriLock stem (52 hips) (DePuy) as tapered wedge stem were enrolled in this study. For preoperative and postoperative evaluation, a CT scan of the pelvis and knee joint was obtained and was transferred to 3D template software. We compared the alignment of preoperative plan for stem anteversion/valgus/anterior tilt angles and postoperative stem alignment, and the absolute error was defined as the surgical error. To clarify the factors contributing to the malalignment or surgical error, we evaluated postoperative stem alignment and several associated factors. Further, we compared the clinical parameters between two types of stems for analysis of the influence of stem type differences.
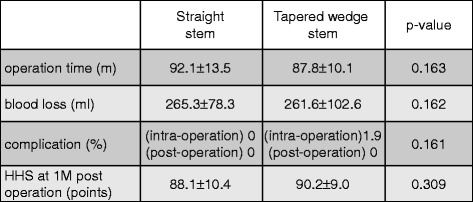
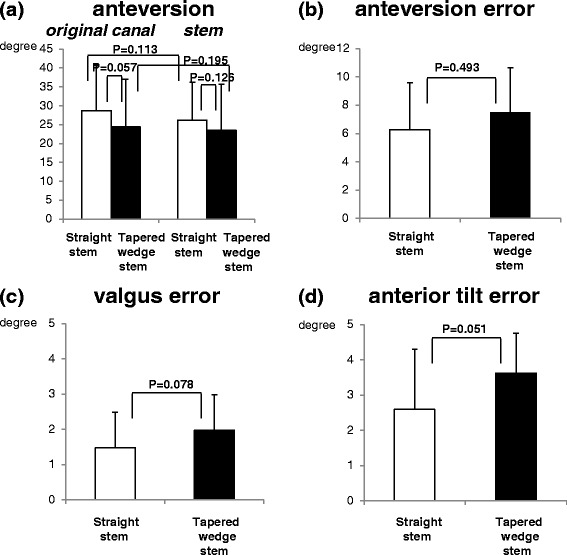
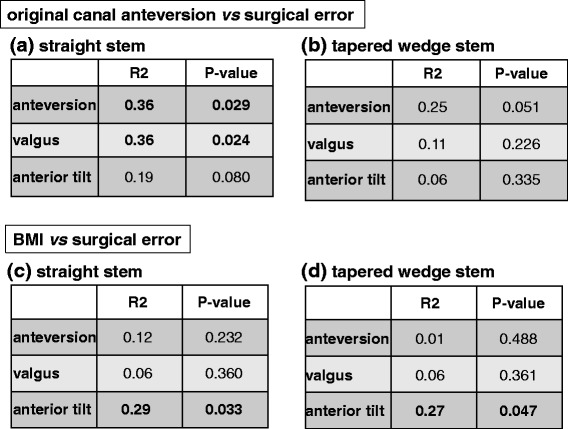
The mean absolute value of the alignment error (postoperative stem alignment-preoperative planning alignment) was not changed in the short tapered wedge and straight stems. Sex, age at operation, or original canal anteversion did not affect the accuracy of stem alignment. However, high body mass index (BMI) affected the accuracy of stem alignment. Clinical outcomes were not changed by the difference of stem types.
The postoperative alignment of short tapered wedge stem was accurate, same as the straight stem during mini-invasive THA, but we need to pay attention when using this in obese patients.
微创外科手术方法广泛应用于全髋关节置换术(THA)。然而,已有报道称手术过程中视野受限会引发一些潜在问题,如植入物位置不当、神经血管损伤和植入物固定不佳。在这些情况下,较短的股骨柄更容易插入股骨髓腔。为了评估较短股骨柄定向的准确性,我们重点关注股骨柄定向的准确性,尤其是短锥形楔形股骨柄,并评估了微创全髋关节置换术中股骨柄排列不齐的影响因素。
本研究纳入了110例接受THA的髋关节,其中58例使用Summit股骨柄(DePuy,华沙,印第安纳州)作为直柄,52例使用TriLock股骨柄(DePuy)作为锥形楔形柄。术前和术后评估时,获取骨盆和膝关节的CT扫描图像并传输至三维模板软件。我们比较了股骨柄前倾角/外翻角/前倾角的术前计划与术后股骨柄排列情况,绝对误差定义为手术误差。为了阐明导致排列不齐或手术误差的因素,我们评估了术后股骨柄排列情况及几个相关因素。此外,我们比较了两种类型股骨柄的临床参数,以分析股骨柄类型差异的影响。
短锥形楔形柄和直柄的排列误差(术后股骨柄排列 - 术前计划排列)的平均绝对值没有变化。性别、手术年龄或原始髓腔前倾角不影响股骨柄排列的准确性。然而,高体重指数(BMI)会影响股骨柄排列的准确性。股骨柄类型的差异并未改变临床结果。
在微创THA中,短锥形楔形柄的术后排列与直柄一样准确,但在肥胖患者中使用时我们需要加以注意。