Taveira-DaSilva Angelo M, Moss Joel
Cardiovascular and Pulmonary Branch, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, USA.
Clin Epidemiol. 2015 Apr 7;7:249-57. doi: 10.2147/CLEP.S50780. eCollection 2015.
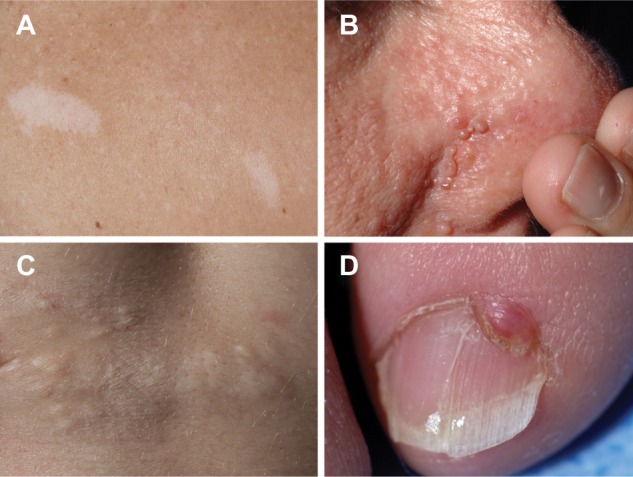
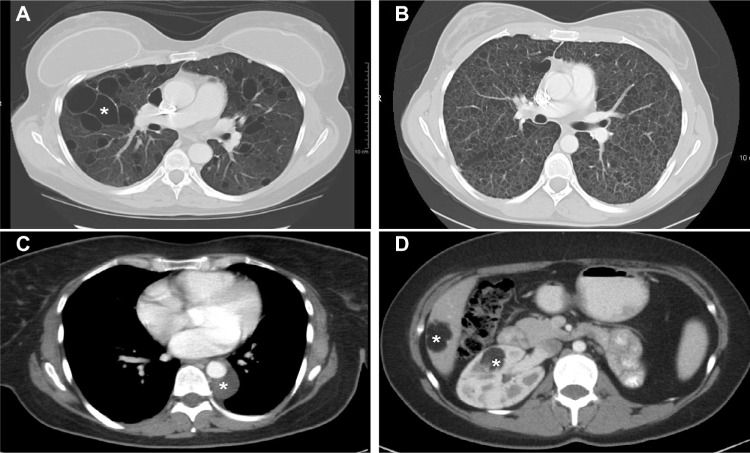
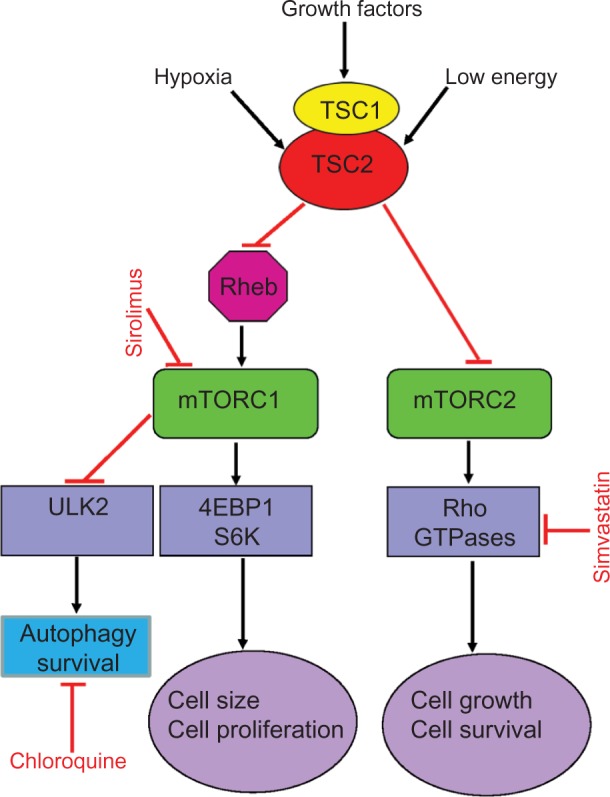
Lymphangioleiomyomatosis (LAM) is a multisystem disease of women, characterized by proliferation of abnormal smooth muscle-like LAM cells, leading to the formation of lung cysts, fluid-filled cystic structures in the axial lymphatics (eg, lymphangioleiomyomas), and renal angiomyolipomas. LAM is caused by mutations of the TSC1 or TSC2 genes, which encode, respectively, hamartin and tuberin, two proteins with a major role in control of the mammalian target of rapamycin (mTOR) signaling pathway. LAM occurs sporadically or in association with tuberous sclerosis complex, an autosomal-dominant syndrome characterized by widespread hamartomatous lesions. LAM may present with progressive dyspnea, recurrent pneumothorax, or chylothorax. Pulmonary function tests show reduced flow rates (forced expiratory volume in the first second) and diffusion capacity. Exercise testing may reveal gas exchange abnormalities, ventilatory limitation, and hypoxemia. The severity and progression of disease may be assessed by lung histology scores, quantification of computed tomography, pulmonary function testing, 6-minute walk tests, cardiopulmonary exercise testing, and measurement of serum vascular endothelial growth factor D levels. Sirolimus and everolimus, two mTOR inhibitors, are effective in stabilizing lung function and reducing the size of chylous effusions, lymphangioleiomyo-mas, and angiomyolipomas. However, inhibition of mTOR complex 1 increases autophagy, possibly enhancing LAM cell survival. Inhibition of autophagy with hydroxychloroquine, in combination with sirolimus, has been proposed as a possible treatment for LAM. Deficiency of tuberin results in increased RhoA GTPase activity and cell survival, an effect that is mediated through mTOR complex 2 signaling. Because sirolimus and everolimus only affect the activity of mTOR complex 1, therapies targeting RhoA GTPases with simvastatin, which inhibits Rho GTPases and promotes apoptosis, are being investigated. As in the case of cancer, LAM may be best treated with multiple drugs targeting signaling pathways considered important in the pathogenesis of disease.
淋巴管平滑肌瘤病(LAM)是一种女性多系统疾病,其特征为异常的平滑肌样LAM细胞增殖,导致肺囊肿形成、轴向淋巴管内出现充满液体的囊性结构(如淋巴管平滑肌瘤)以及肾血管平滑肌脂肪瘤。LAM由TSC1或TSC2基因的突变引起,这两个基因分别编码错构瘤蛋白和结节蛋白,这两种蛋白在控制哺乳动物雷帕霉素靶蛋白(mTOR)信号通路中起主要作用。LAM可散发出现或与结节性硬化症相关,结节性硬化症是一种常染色体显性综合征,其特征为广泛的错构瘤性病变。LAM可能表现为进行性呼吸困难、复发性气胸或乳糜胸。肺功能测试显示流速(第一秒用力呼气量)和弥散能力降低。运动测试可能揭示气体交换异常、通气受限和低氧血症。疾病的严重程度和进展可通过肺组织学评分、计算机断层扫描定量、肺功能测试、6分钟步行测试、心肺运动测试以及血清血管内皮生长因子D水平的测量来评估。西罗莫司和依维莫司这两种mTOR抑制剂,在稳定肺功能以及减小乳糜性胸腔积液、淋巴管平滑肌瘤和血管平滑肌脂肪瘤的大小方面有效。然而,抑制mTOR复合物1会增加自噬,可能会提高LAM细胞的存活率。有人提出用羟氯喹抑制自噬并联合西罗莫司作为LAM的一种可能治疗方法。结节蛋白的缺乏会导致RhoA GTP酶活性增加和细胞存活,这种效应是通过mTOR复合物2信号传导介导的。由于西罗莫司和依维莫司仅影响mTOR复合物1的活性,因此正在研究用辛伐他汀靶向RhoA GTP酶的疗法,辛伐他汀可抑制Rho GTP酶并促进细胞凋亡。与癌症情况一样,LAM可能最好用多种靶向疾病发病机制中被认为重要的信号通路的药物进行治疗。