van Nies Jessica A B, Alves Celina, Radix-Bloemen Audrey L S, Gaujoux-Viala Cécile, Huizinga Tom W J, Hazes Johanna M W, Brouwer Elisabeth, Fautrel Bruno, van der Helm-van Mil Annette H M
Department of Rheumatology, Leiden University Medical Center, Albinusdreef 2, 2333 ZC, Leiden, the Netherlands.
Department of Rheumatology, Erasmus MC, University Medical Center Rotterdam, 's-Gravendijkwal 230, 3015 CE, Rotterdam, the Netherlands.
Arthritis Res Ther. 2015 Apr 23;17(1):108. doi: 10.1186/s13075-015-0616-3.
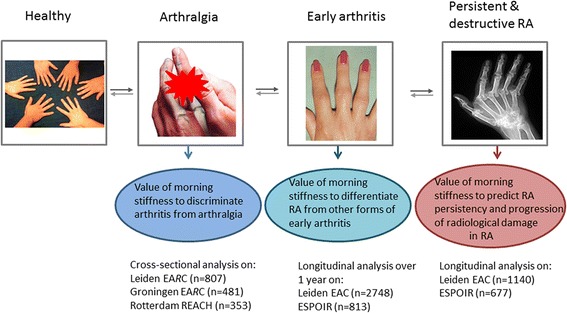
Morning stiffness is assessed daily in the diagnostic process of arthralgia and arthritis, but large-scale studies on the discriminative ability are absent. This study explored the diagnostic value of morning stiffness in 5,202 arthralgia and arthritis patients and the prognostic value in early rheumatoid arthritis (RA).
In arthralgia patients referred to the Early Arthritis Recognition Clinics (EARC) of Leiden (n = 807) and Groningen (n = 481) or included in the Rotterdam Early Arthritis Cohort (REACH) study (n = 353), the associations (cross-sectional analyses) between morning stiffness and presence of arthritis at physical examination were studied. In early arthritis patients, included in the Leiden Early Arthritis Clinic (EAC) (n = 2,748) and Evaluation et Suivi de POlyarthrites Indifférenciées Récentes (ESPOIR) (n = 813), associations with fulfilling the 2010-RA criteria after one year were assessed. In 2010-RA patients included in the EAC (n = 1,140) and ESPOIR (n = 677), association with the long-term outcomes of disease-modifying antirheumatic drug (DMARD)-free sustained remission and radiological progression were determined. Morning stiffness was defined as a duration ≥60 minutes; sensitivity analyses were performed for other definitions.
In arthralgia, morning stiffness (≥60 minutes) associated with the presence of arthritis; Leiden EARC odds ratio (OR) 1.49 (95% CI 1.001 to 2.20), Groningen EARC OR 2.21 (1.33 to 3.69) and REACH OR 1.55 (0.97 to 2.47) but the areas under the receiver operating characteristic curve (AUCs) were low (0.52, 0.57, 0.54). In early arthritis, morning stiffness was associated with 2010-RA independent of other predictors (Leiden EAC OR 1.72 (95% CI 1.31 to 2.25, AUC 0.68), ESPOIR OR 1.68 (1.03 to 2.74, AUC 0.64)). Duration of ≥30 minutes provided optimal discrimination for RA in early arthritis. Morning stiffness was not associated with radiological progression or DMARD-free sustained remission.
Morning stiffness in arthralgia and early arthritis is associated with arthritis and RA respectively. This supports the incorporation of morning stiffness in the diagnostic process.
在关节痛和关节炎的诊断过程中,每天都会评估晨僵情况,但缺乏关于其鉴别能力的大规模研究。本研究探讨了晨僵在5202例关节痛和关节炎患者中的诊断价值以及在早期类风湿关节炎(RA)中的预后价值。
在转诊至莱顿(n = 807)和格罗宁根(n = 481)早期关节炎识别诊所(EARC)或纳入鹿特丹早期关节炎队列(REACH)研究(n = 353)的关节痛患者中,研究晨僵与体格检查时关节炎存在之间的关联(横断面分析)。在纳入莱顿早期关节炎诊所(EAC)(n = 2748)和新发多关节炎评估与随访(ESPOIR)(n = 813)的早期关节炎患者中,评估与一年后符合2010年RA标准之间的关联。在纳入EAC(n = 1140)和ESPOIR(n = 677)的2010年RA患者中,确定与无改善病情抗风湿药(DMARD)持续缓解和放射学进展的长期结局之间的关联。晨僵定义为持续时间≥60分钟;对其他定义进行了敏感性分析。
在关节痛患者中,晨僵(≥60分钟)与关节炎的存在相关;莱顿EARC的比值比(OR)为1.49(95%可信区间1.001至2.20),格罗宁根EARC的OR为2.21(1.33至3.69),REACH的OR为1.55(0.97至2.47),但受试者工作特征曲线下面积(AUC)较低(0.52、0.57、0.54)。在早期关节炎患者中,晨僵与2010年RA相关,独立于其他预测因素(莱顿EAC的OR为1.72(95%可信区间1.31至2.25,AUC为0.68),ESPOIR的OR为1.68(1.03至2.74,AUC为0.64))。持续时间≥30分钟对早期关节炎中的RA具有最佳鉴别能力。晨僵与放射学进展或无DMARD持续缓解无关。
关节痛和早期关节炎中的晨僵分别与关节炎和RA相关。这支持将晨僵纳入诊断过程。