Emergency and Critical Care Center, Hokkaido University Hospital, N14W5, Kita-ku, Sapporo, 060-8648 Japan.
Department of Traumatology and Critical Care Medicine, Sapporo Medical University Hospital, Sapporo, Japan.
J Intensive Care. 2013 Dec 4;1(1):12. doi: 10.1186/2052-0492-1-12. eCollection 2013.
Epinephrine administration has been advocated for cardiopulmonary resuscitation (CPR) for decades. Despite the fact that epinephrine administration during CPR is internationally accepted, the effects of the prehospital epinephrine administration still remain controversial. We investigated the effects of epinephrine administration on patients with out-of-hospital cardiac arrest based on a propensity analysis with regard to the 'CPR time'.
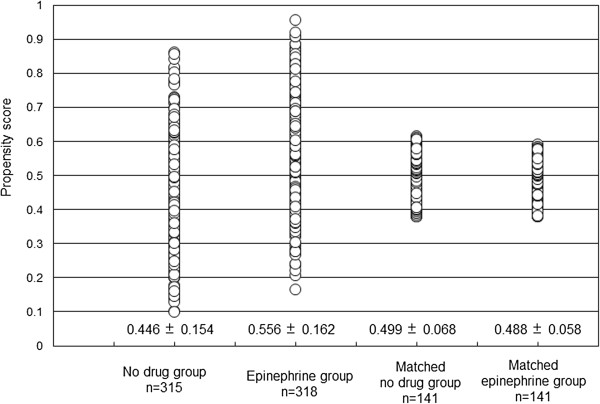
From April 1, 2007, to December 31, 2009, 633 out-of-hospital cardiac arrest patients with bystander witnesses were included in the present study. To rule out any survival bias, we used the propensity scores, which included CPR time. CPR time was defined as the time span from when the emergency medical technicians started CPR until either the return of spontaneous circulation or arrival at the hospital. After performing propensity score matching, the epinephrine and no-drug groups each included 141 patients. The primary study endpoint was a favorable neurological outcome at 30 days after cardiac arrest.
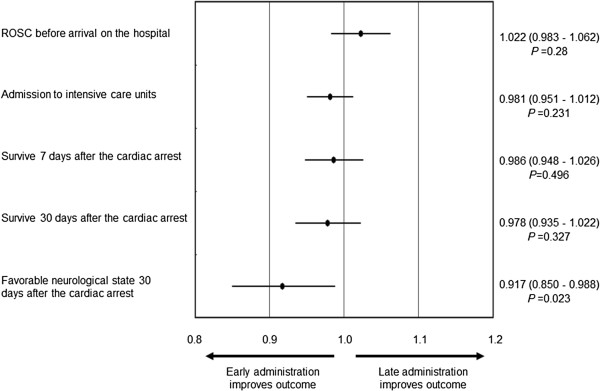
After propensity score matching, the frequency of the return of spontaneous circulation before arrival at the hospital in the matched epinephrine group was higher than that in the matched no-drug group (27% vs. 13%, P = 0.002). However, the frequency of a favorable neurological state did not differ between the two groups. With regard to the frequency of a favorable neurological state in the patients, the adjusted odds ratio of the time span from cardiac arrest to the first epinephrine administration was 0.917 (95% confidence interval 0.850-0.988, P = 0.023) per minute.
In patients with witnessed out-of-hospital cardiac arrest, prehospital epinephrine administration was associated with increase of the return of spontaneous circulation before arrival at the hospital. Moreover, the early administration of epinephrine might improve the overall neurological outcome.
几十年来,肾上腺素的给药一直被提倡用于心肺复苏(CPR)。尽管在 CPR 期间给予肾上腺素给药在国际上得到认可,但院前肾上腺素给药的效果仍然存在争议。我们根据“CPR 时间”进行了倾向分析,研究了肾上腺素给药对院外心脏骤停患者的影响。
从 2007 年 4 月 1 日至 2009 年 12 月 31 日,本研究纳入了 633 名有旁观者见证的院外心脏骤停患者。为了排除任何生存偏见,我们使用了包括 CPR 时间在内的倾向评分。CPR 时间定义为从急救人员开始 CPR 到自主循环恢复或到达医院的时间跨度。进行倾向评分匹配后,肾上腺素组和无药物组各包括 141 例患者。主要研究终点是心脏骤停后 30 天的良好神经功能预后。
经过倾向评分匹配后,匹配的肾上腺素组在到达医院前自主循环恢复的频率高于匹配的无药物组(27%比 13%,P=0.002)。然而,两组之间的良好神经状态的频率没有差异。对于两组患者良好神经状态的频率,从心脏骤停到第一次肾上腺素给药的时间间隔的调整优势比为 0.917(95%置信区间 0.850-0.988,P=0.023)每分钟。
在有目击者的院外心脏骤停患者中,院前肾上腺素给药与到达医院前自主循环恢复的增加相关。此外,早期给予肾上腺素可能改善整体神经功能预后。