de Jager Pieter, Chirwa Tobias, Naidoo Shan, Perovic Olga, Thomas Juno
Epidemiology and Surveillance Unit, National Institute for Occupational Health, National Health Laboratory Service, Johannesburg, South Africa; Department of Community Health, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Department of Epidemiology and Biostatistics, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
PLoS One. 2015 Apr 24;10(4):e0123337. doi: 10.1371/journal.pone.0123337. eCollection 2015.
New Delhi metallo-β-lactamase (NDM)-producing Gram-negative bacteria have spread globally and pose a significant public health threat. There is a need to better define risk factors and outcomes of NDM-1 clinical infection. We assessed risk factors for nosocomial infection with NDM-1-producers and associated in-hospital mortality.
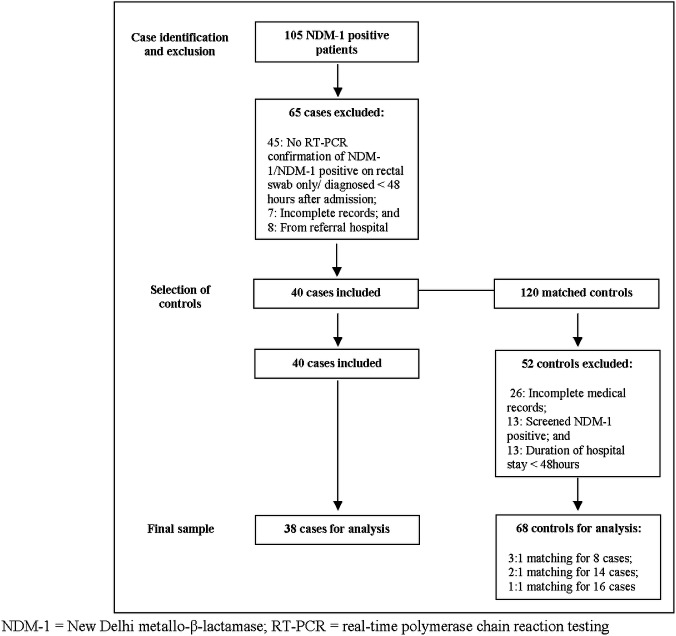
A matched case-control study was conducted during a nosocomial outbreak of NDM-1-producers in an adult intensive care unit (ICU) in South Africa. All patients from whom NDM-1-producers were identified were considered (n=105). Cases included patients admitted during the study period in whom NDM-1 producing Gram-negative bacteria were isolated from clinical specimens collected ≥48 hours after admission, and where surveillance definitions for healthcare-associated infections were met. Controls were matched for age, sex, date of hospital admission and intensive-care admission. Conditional logistic regression was used to identify risk factors for NDM-1 clinical infection and associated in-hospital mortality.
38 cases and 68 controls were included. Klebsiella pneumoniae was the most common NDM-1-producer (28/38, 74%). Cases had longer mean hospital stays (44.0 vs. 13.3 days; P < 0.001) and ICU stays (32.5 vs. 8.3 days; P < 0.001). Adjusting for co-morbid disease, the in-hospital mortality of cases was significantly higher than controls (55.3% vs. 14.7%; AOR, 11.29; P < 0.001). Higher Charlson co-morbidity index score (5.2 vs. 4.1; AOR, 1.59; P = 0.005), mechanical ventilation days (7.47 vs. 0.94 days; AOR, 1.32; P = 0.003) and piperacillin/tazobactam exposure (11.03 vs. 1.05 doses; AOR, 1.08; P = 0.013) were identified as risk factors on multivariate analysis. Cases had a significantly higher likelihood of in-hospital mortality when the NDM-1-producer was Klebsiella pneumoniae (AOR, 16.57; P = 0.007), or when they had a bloodstream infection (AOR, 8.84; P = 0.041).
NDM-1 infection is associated with significant in-hospital mortality. Risk factors for hospital-associated infection include the presence of co-morbid disease, mechanical ventilation and piperacillin/tazobactam exposure.
产新德里金属β-内酰胺酶(NDM)的革兰氏阴性菌已在全球范围内传播,对公众健康构成重大威胁。有必要更好地界定NDM-1临床感染的危险因素和结局。我们评估了NDM-1产菌所致医院感染的危险因素及相关的院内死亡率。
在南非一家成人重症监护病房(ICU)发生的NDM-1产菌医院感染暴发期间进行了一项配对病例对照研究。所有被鉴定出产NDM-1菌的患者均纳入研究(n = 105)。病例包括在研究期间入院、入院≥48小时后从临床标本中分离出产NDM-1的革兰氏阴性菌且符合医疗保健相关感染监测定义的患者。对照在年龄、性别、入院日期和重症监护病房入院日期方面进行匹配。采用条件逻辑回归来确定NDM-1临床感染的危险因素及相关的院内死亡率。
纳入38例病例和68例对照。肺炎克雷伯菌是最常见的产NDM-1菌(28/38,74%)。病例的平均住院时间更长(44.0天对13.3天;P < 0.001),ICU住院时间也更长(32.5天对8.3天;P < 0.001)。校正合并疾病后,病例的院内死亡率显著高于对照(55.3%对14.7%;比值比[AOR],11.29;P < 0.001)。多因素分析确定较高的查尔森合并症指数评分(5.2对4.1;AOR,1.59;P = < 0.005)、机械通气天数(7.47天对0.94天;AOR,1.32;P = 0.003)和哌拉西林/他唑巴坦暴露量(11.03剂对1.05剂;AOR,1.08;P = 0.013)为危险因素。当产NDM-1菌为肺炎克雷伯菌时(AOR,16.57;P = 0.007),或病例发生血流感染时(AOR,8.84;P = 0.041),其院内死亡的可能性显著更高。
NDM-1感染与显著的院内死亡率相关。医院相关感染的危险因素包括合并疾病的存在、机械通气和哌拉西林/他唑巴坦暴露。