Leppert Wojciech
Chair and Department of Palliative Medicine, Poznan University of Medical Sciences, Poznan, Poland.
Drug Des Devel Ther. 2015 Apr 16;9:2215-31. doi: 10.2147/DDDT.S32684. eCollection 2015.
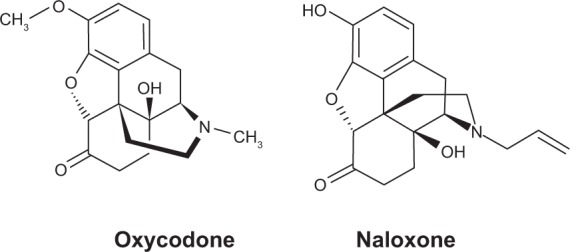
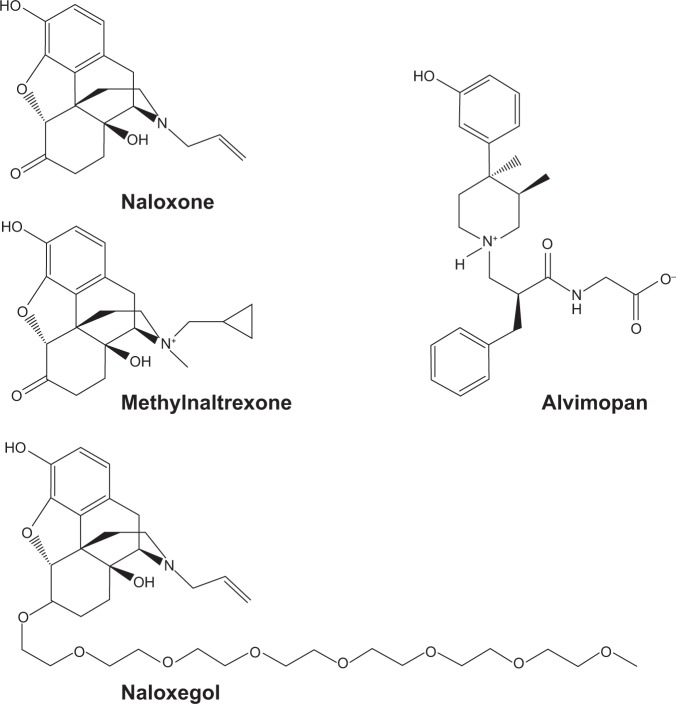
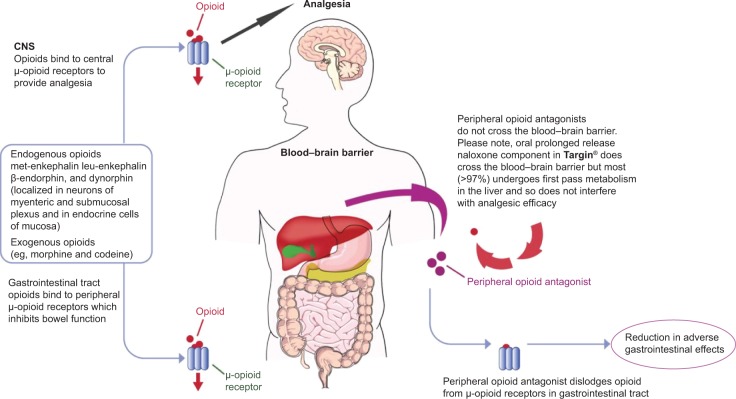
Opioid-induced bowel dysfunction (OIBD) comprises gastrointestinal (GI) symptoms, including dry mouth, nausea, vomiting, gastric stasis, bloating, abdominal pain, and opioid-induced constipation, which significantly impair patients' quality of life and may lead to undertreatment of pain. Traditional laxatives are often prescribed for OIBD symptoms, although they display limited efficacy and exert adverse effects. Other strategies include prokinetics and change of opioids or their administration route. However, these approaches do not address underlying causes of OIBD associated with opioid effects on mostly peripheral opioid receptors located in the GI tract. Targeted management of OIBD comprises purely peripherally acting opioid receptor antagonists and a combination of opioid receptor agonist and antagonist. Methylnaltrexone induces laxation in 50%-60% of patients with advanced diseases and OIBD who do not respond to traditional oral laxatives without inducing opioid withdrawal symptoms with similar response (45%-50%) after an oral administration of naloxegol. A combination of prolonged-release oxycodone with prolonged-release naloxone (OXN) in one tablet (a ratio of 2:1) provides analgesia with limited negative effect on the bowel function, as oxycodone displays high oral bioavailability and naloxone demonstrates local antagonist effect on opioid receptors in the GI tract and is totally inactivated in the liver. OXN in daily doses of up to 80 mg/40 mg provides equally effective analgesia with improved bowel function compared to oxycodone administered alone in patients with chronic non-malignant and cancer-related pain. OIBD is a common complication of long-term opioid therapy and may lead to quality of life deterioration and undertreatment of pain. Thus, a complex assessment and management that addresses underlying causes and patomechanisms of OIBD is recommended. Newer strategies comprise methylnaltrexone or OXN administration in the management of OIBD, and OXN may be also considered as a preventive measure of OIBD development in patients who require opioid administration.
阿片类药物引起的肠道功能障碍(OIBD)包括胃肠道(GI)症状,如口干、恶心、呕吐、胃潴留、腹胀、腹痛以及阿片类药物引起的便秘,这些症状会显著损害患者的生活质量,并可能导致疼痛治疗不足。尽管传统泻药对OIBD症状的疗效有限且会产生不良反应,但仍经常被用于治疗OIBD。其他策略包括促动力药以及更换阿片类药物或其给药途径。然而,这些方法并未解决与阿片类药物对主要位于胃肠道的外周阿片受体的作用相关的OIBD根本原因。OIBD的靶向治疗包括纯粹的外周作用阿片受体拮抗剂以及阿片受体激动剂和拮抗剂的联合使用。甲基纳曲酮可使50%-60%患有晚期疾病且对传统口服泻药无反应的OIBD患者产生通便作用,且不会诱发阿片类药物戒断症状,口服纳洛西酮后也有类似的反应(45%-50%)。缓释羟考酮与缓释纳洛酮(OXN)以1片(比例为2:1)的形式联合使用可提供镇痛作用,且对肠道功能的负面影响有限,因为羟考酮具有较高的口服生物利用度,而纳洛酮对胃肠道中的阿片受体具有局部拮抗作用,并且在肝脏中完全失活。与单独使用羟考酮相比,每日剂量高达80 mg/40 mg的OXN在慢性非恶性和癌症相关疼痛患者中提供了同样有效的镇痛作用,同时改善了肠道功能。OIBD是长期阿片类药物治疗的常见并发症,可能导致生活质量下降和疼痛治疗不足。因此,建议进行综合评估和管理,以解决OIBD的根本原因和发病机制。新的策略包括在OIBD管理中使用甲基纳曲酮或OXN,对于需要使用阿片类药物的患者,OXN也可被视为预防OIBD发生的措施。