Lee Karla C L, Baker Luisa A, Stanzani Giacomo, Alibhai Hatim, Chang Yu Mei, Jimenez Palacios Carolina, Leckie Pamela J, Giordano Paola, Priestnall Simon L, Antoine Daniel J, Jenkins Rosalind E, Goldring Christopher E, Park B Kevin, Andreola Fausto, Agarwal Banwari, Mookerjee Rajeshwar P, Davies Nathan A, Jalan Rajiv
Department of Clinical Science and Services, The Royal Veterinary College, Hertfordshire, UK.
Department of Clinical Science and Services, The Royal Veterinary College, Hertfordshire, UK.
J Hepatol. 2015 Sep;63(3):634-42. doi: 10.1016/j.jhep.2015.04.020. Epub 2015 May 1.
BACKGROUND & AIMS: In acute liver failure, severity of liver injury and clinical progression of disease are in part consequent upon activation of the innate immune system. Endotoxaemia contributes to innate immune system activation and the detoxifying function of albumin, critical to recovery from liver injury, is irreversibly destroyed in acute liver failure. University College London-Liver Dialysis Device is a novel artificial extracorporeal liver assist device, which is used with albumin infusion, to achieve removal and replacement of dysfunctional albumin and reduction in endotoxaemia. We aimed to test the effect of this device on survival in a pig model of acetaminophen-induced acute liver failure.
Pigs were randomised to three groups: Acetaminophen plus University College London-Liver Dialysis Device (n=9); Acetaminophen plus Control Device (n=7); and Control plus Control Device (n=4). Device treatment was initiated two h after onset of irreversible acute liver failure.
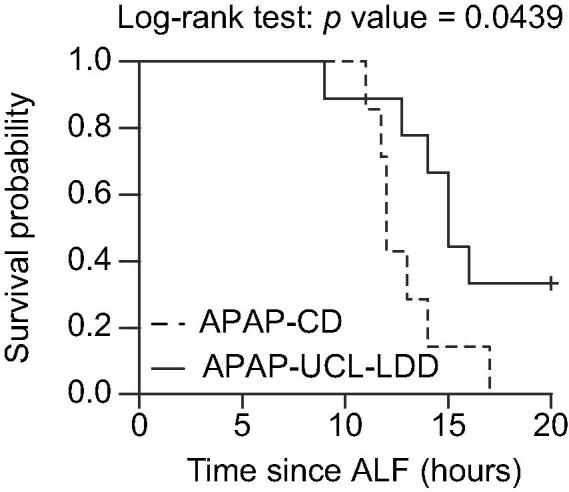
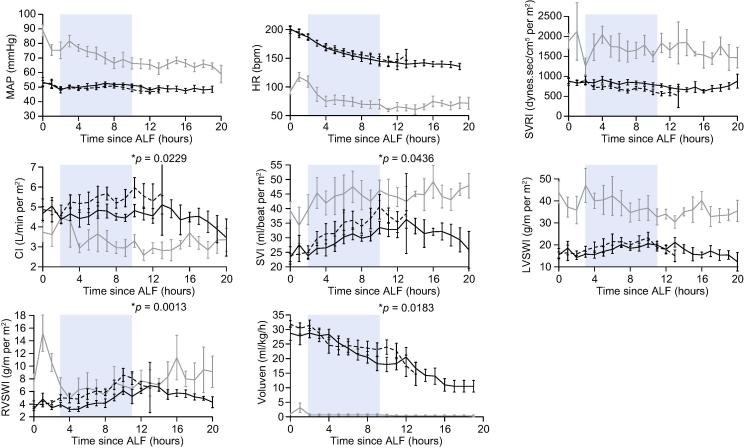
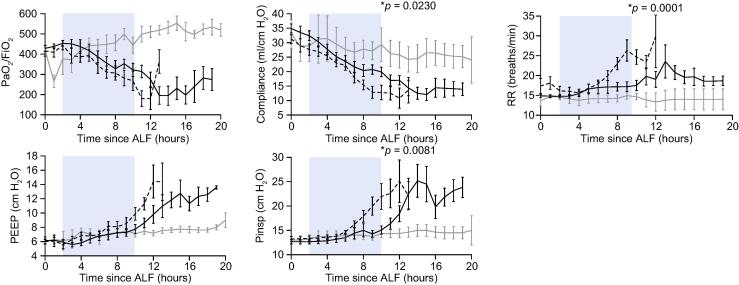
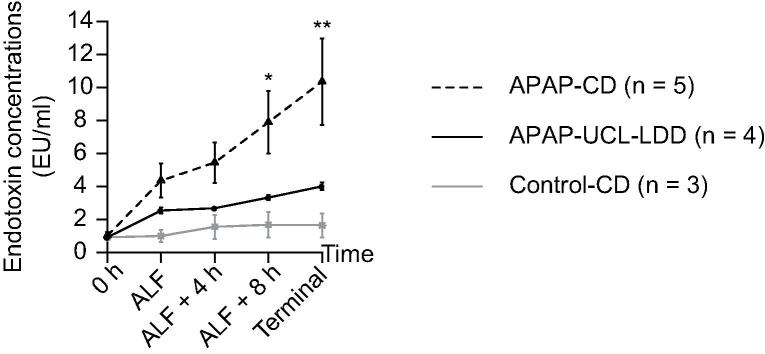
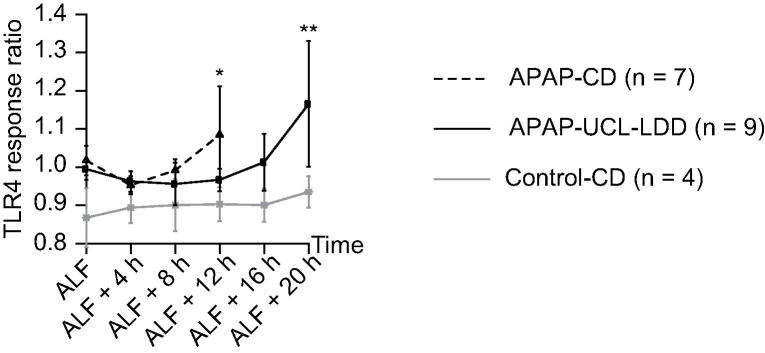
The Liver Dialysis Device resulted in 67% reduced risk of death in acetaminophen-induced acute liver failure compared to Control Device (hazard ratio=0.33, p=0.0439). This was associated with 27% decrease in circulating irreversibly oxidised human non-mercaptalbumin-2 throughout treatment (p=0.046); 54% reduction in overall severity of endotoxaemia (p=0.024); delay in development of vasoplegia and acute lung injury; and delay in systemic activation of the TLR4 signalling pathway. Liver Dialysis Device-associated adverse clinical effects were not seen.
The survival benefit and lack of adverse effects would support clinical trials of University College London-Liver Dialysis Device in acute liver failure patients.
在急性肝衰竭中,肝损伤的严重程度和疾病的临床进展部分归因于先天免疫系统的激活。内毒素血症促成先天免疫系统激活,而白蛋白的解毒功能对肝损伤的恢复至关重要,在急性肝衰竭中会被不可逆地破坏。伦敦大学学院肝脏透析装置是一种新型人工体外肝辅助装置,与白蛋白输注联合使用,以实现去除和替代功能失调的白蛋白并降低内毒素血症。我们旨在测试该装置对乙酰氨基酚诱导的急性肝衰竭猪模型生存的影响。
将猪随机分为三组:乙酰氨基酚加伦敦大学学院肝脏透析装置组(n = 9);乙酰氨基酚加对照装置组(n = 7);以及对照组加对照装置组(n = 4)。在不可逆性急性肝衰竭发作两小时后开始装置治疗。
与对照装置相比,肝脏透析装置使乙酰氨基酚诱导的急性肝衰竭死亡风险降低了67%(风险比 = 0.33,p = 0.0439)。这与整个治疗过程中循环中不可逆氧化的人非巯基白蛋白 - 2降低27%相关(p = 0.046);内毒素血症总体严重程度降低54%(p = 0.024);血管麻痹和急性肺损伤的发生延迟;以及TLR4信号通路的全身激活延迟。未观察到与肝脏透析装置相关的不良临床影响。
生存获益和无不良反应支持对伦敦大学学院肝脏透析装置在急性肝衰竭患者中进行临床试验。