Butt Thomas, Lee Aaron, Lee Cecilia, Tufail Adnan
Institute of Ophthalmology, University College London, London, UK.
Moorfields Eye Hospital, London, UK.
BMJ Open. 2015 May 5;5(5):e006535. doi: 10.1136/bmjopen-2014-006535.
To evaluate the cost-effectiveness of immediate treatment with ranibizumab in patients with neovascular age-related macular degeneration (nAMD) with good (better than 6/12) starting visual acuity compared with current UK clinical guidance of waiting until vision falls below 6/12 to begin treatment, using real-world outcomes data.
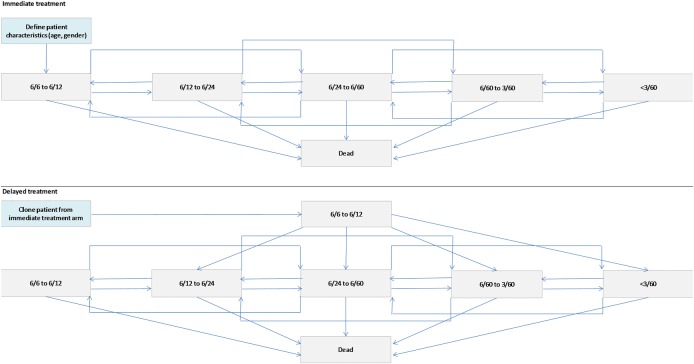
A patient-level health economic state transition model based on levels of visual acuity in the better seeing eye was constructed to simulate the costs and consequences of treating patients with nAMD with ranibizumab.
The model took the perspective of the UK National Health Service (NHS).
The model was populated with real-world outcomes and resource use from a prospective multicentre national nAMD database study containing 92,976 ranibizumab treatment episodes.
Two treatment approaches were compared: immediate intervention with 0.5 mg ranibizumab pro re nata, PRN (on detection of nAMD) or delayed intervention (waiting until vision fell to 6/12 before beginning treatment).
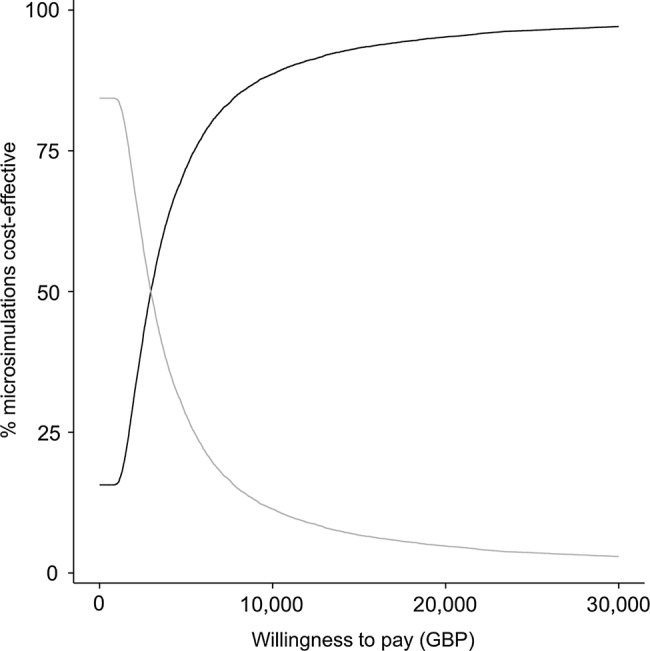
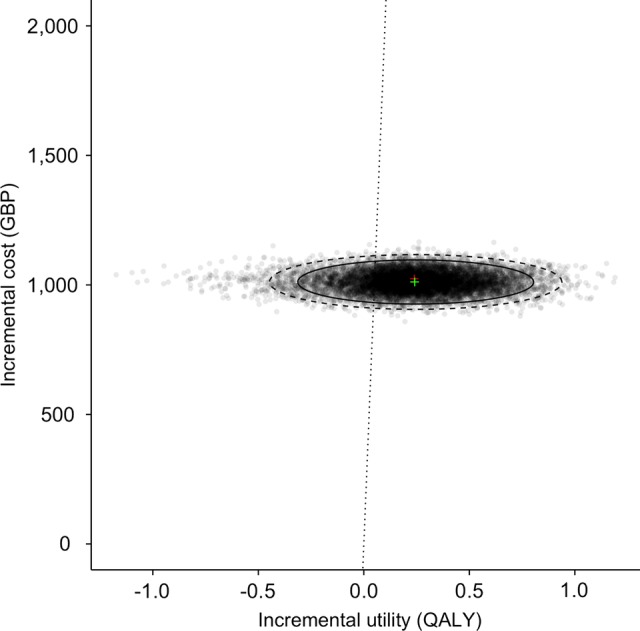
Quality-adjusted life years (QALYs) for health states and healthcare costs were accrued for each strategy, and an incremental cost-effectiveness ratio (ICER) was calculated. One-way and probabilistic sensitivity analyses were employed to test the uncertainty of the model.
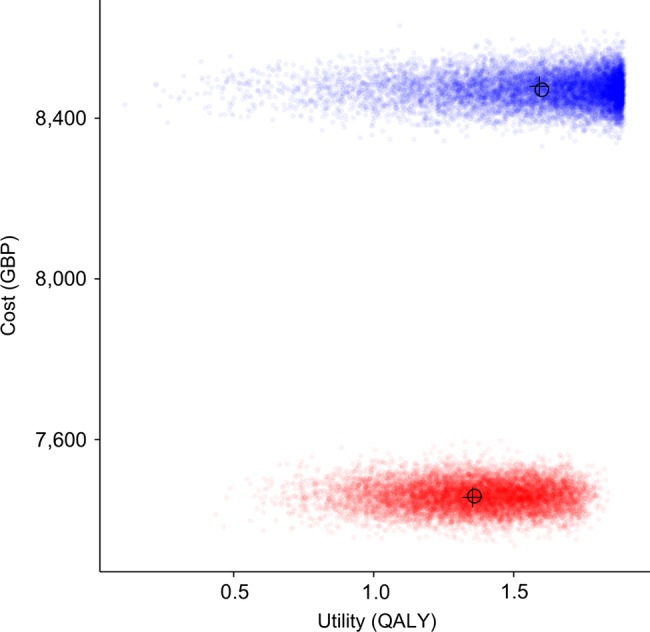
Over a 2-year time horizon, based on 10,000 Monte Carlo simulations, the early treatment arm accumulated 1.59 QALYs and £8469.79 cost. The delayed treatment arm accumulated 1.35 QALYs and £7460.21 cost. The central ICER estimate was £4251.60.
A model based on real-world data is likely to be a realistic reflection of the health gains and resource use of ranibizumab for nAMD in the UK NHS. Initiating treatment immediately with ranibizumab PRN regimen is a cost-effective strategy compared with current guidance of initiating treatment at a level of 6/12 or worse vision.
与英国当前临床指南(即等到视力降至6/12以下才开始治疗)相比,利用真实世界结局数据,评估雷珠单抗即刻治疗对起始视力良好(优于6/12)的新生血管性年龄相关性黄斑变性(nAMD)患者的成本效益。
构建了一个基于较好眼视力水平的患者层面健康经济状态转换模型,以模拟用雷珠单抗治疗nAMD患者的成本和后果。
该模型采用了英国国家医疗服务体系(NHS)的视角。
该模型纳入了一项前瞻性多中心全国性nAMD数据库研究中的真实世界结局和资源使用情况,该研究包含92,976次雷珠单抗治疗事件。
比较了两种治疗方法:0.5mg雷珠单抗按需给药(PRN,在检测到nAMD时)即刻干预或延迟干预(等到视力降至6/12才开始治疗)。
为每种策略计算健康状态的质量调整生命年(QALYs)和医疗保健成本,并计算增量成本效益比(ICER)。采用单向和概率敏感性分析来检验模型的不确定性。
在2年的时间范围内,基于10,000次蒙特卡洛模拟,早期治疗组累积1.59个QALYs和8469.79英镑的成本。延迟治疗组累积1.35个QALYs和7460.21英镑的成本。ICER的中心估计值为4251.60英镑。
基于真实世界数据的模型可能真实反映了在英国NHS中雷珠单抗治疗nAMD的健康获益和资源使用情况。与当前在视力为6/12或更差时开始治疗的指南相比,雷珠单抗PRN方案即刻开始治疗是一种具有成本效益的策略。