Ungar Bella, Haj-Natour Ola, Kopylov Uri, Yavzori Miri, Fudim Ella, Picard Orit, Loebstein Ronen, Lahat Adi, Maor Yaakov, Avidan Benjamin, Lang Alon, Weiss Batia, Chowers Yehuda, Eliakim Rami, Ben-Horin Shomron
From the Department of Gastroenterology, Sheba Medical Center Tel Hashomer (BU, OH-N, UK, MY, EF, OP, AL, YM, BA, AL, RE, SB-H); Institute of Clinical Pharmacology, Sheba Medical Center Tel Hashomer (RL); Pediatric Gastroenterology Unit, Edmond & Lily Safra Children's Hospital Tel Hashomer (BW); Sackler School of Medicine, Tel-Aviv University (BU, OH-N, UK, MY, EF, OP, RL, AL, YM, BA, AL, BW, RE, SB-H); and Rambam Health Care Campus & Bruce Rappaport School of Medicine, Technion Institute of Technology, Haifa, Israel (YC).
Medicine (Baltimore). 2015 May;94(18):e673. doi: 10.1097/MD.0000000000000673.
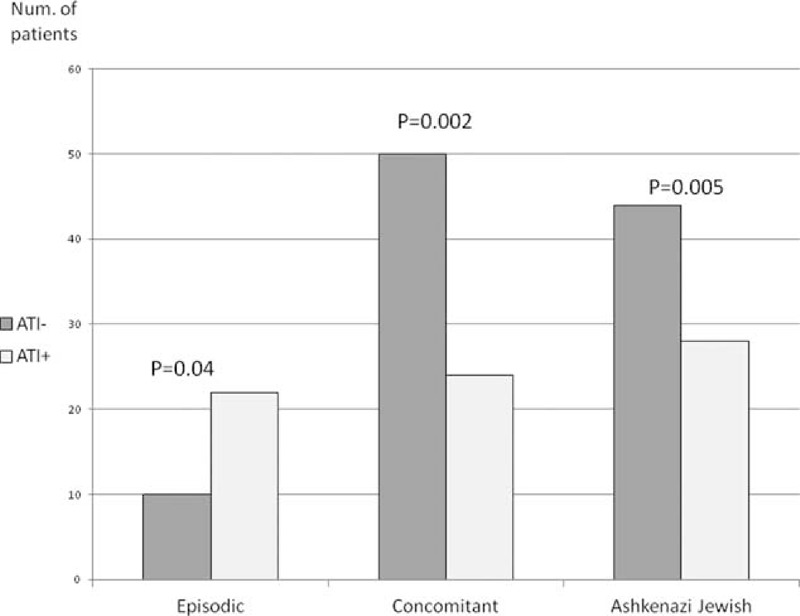
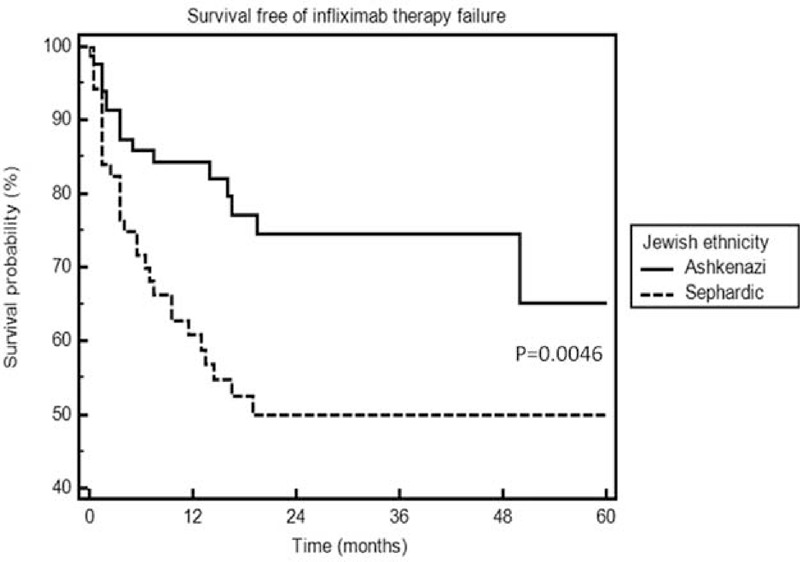
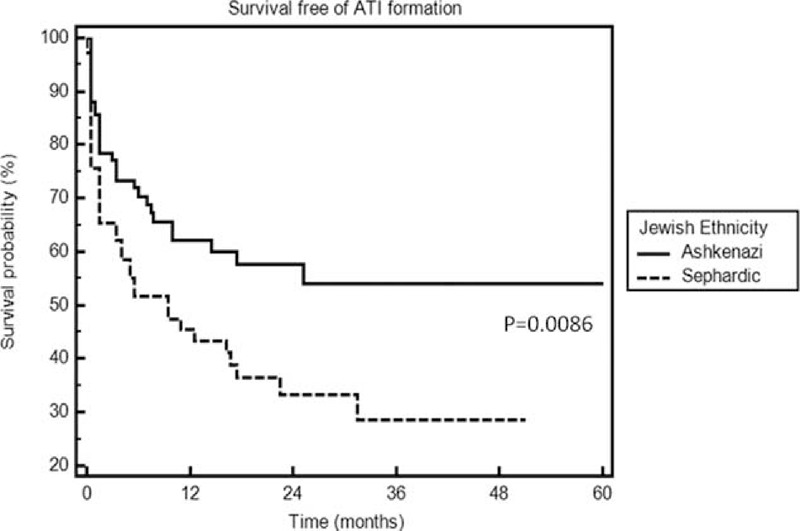
Infliximab is an anti-tumor necrosis factor (TNF) used for treatment of inflammatory bowel disease (IBD) as well as rheumatoid arthritis, psoriasis, and other inflammatory conditions. Antibodies to infliximab (ATI) develop in approximately 45% of infliximab-treated IBD patients and are correlated with loss of clinical response. Scarce data exist as to factors which predict infliximab immunogenicity.To investigate factors that may predict formation of antibodies to infliximab (ATI) and infliximab therapy failure an observational study of consecutive IBD patients treated with infliximab between 2009 and 2013 was performed. Trough levels of ATI were measured. Patients were monitored for disease activity using clinical activity indexes and were classified according to ATI formation and clinical response. All clinical and demographic parameters were analyzed for association with the designated outcomes.One hundred fifty-nine patients were included and 1505 sera were tested. On multivariate analysis, Jewish Ashkenazi ethnicity was protective against both development of ATI (odds ratio [OR] 0.35, 95% confidence interval [CI] 0.17-0.7, P = 0.005) and treatment failure (OR 0.29, 95% CI 0.13-0.66, P = 0.003). Concomitant immunomodulator therapy was also negatively associated with immunogenicity and infliximab therapy failure (OR 0.31, 95% CI 0.15-0.65, P = 0.002; OR 0.42 95% CI 0.18-0.99, p = 0.04, respectively), whereas episodic therapy was positively associated with both outcomes (OR 4.2 95% CI 1.07-16.1, p = 0.04, OR 4.45 95% CI 1.2-16.6, p = 0.026 respectively). All other variables, including IBD type, gender, weight, age, smoking status and disease duration, were not predictive of ATI formation or clinical failure. However, among Crohn's disease patients, a non-stricturing non-penetrating phenotype was protective against ATI formation (OR 0.4, 95% CI 0.14-0.96, p = 0.04). P = 0.04, respectively), whereas episodic/interrupted therapy was positively associated with both outcomes (OR 4.2, 95% CI 1.07-16.1, P = 0.04; OR 4.45, 95% CI 1.2-16.6, P = 0.026, respectively). All other variables, including IBD type, sex, weight, age, smoking status, and disease duration, were not predictive of ATI formation or clinical failure. However, among Crohn disease patients, a nonstricturing nonpenetrating phenotype was protective against ATI formation (OR 0.4, 95% CI 0.14-0.96, P = 0.04).Jewish Ashkenazi ethnicity is protective of ATI formation and infliximab therapy failure. These findings suggest a role for ethnicity, and implicitly for genetic predisposition, in modulating the risk of anti-TNF immunogenicity and treatment unresponsiveness.
英夫利昔单抗是一种抗肿瘤坏死因子(TNF)药物,用于治疗炎症性肠病(IBD)以及类风湿性关节炎、银屑病和其他炎症性疾病。在接受英夫利昔单抗治疗的IBD患者中,约45%会产生抗英夫利昔单抗抗体(ATI),且这与临床反应丧失相关。关于预测英夫利昔单抗免疫原性的因素,现有数据稀少。为了研究可能预测抗英夫利昔单抗抗体(ATI)形成及英夫利昔单抗治疗失败的因素,我们对2009年至2013年间连续接受英夫利昔单抗治疗的IBD患者进行了一项观察性研究。测量了ATI的谷浓度。使用临床活动指数对患者的疾病活动进行监测,并根据ATI形成情况和临床反应进行分类。分析所有临床和人口统计学参数与指定结局的相关性。共纳入159例患者,检测了1505份血清。多因素分析显示,犹太阿什肯纳兹族裔对ATI形成(比值比[OR]0.35,95%置信区间[CI]0.17 - 0.7,P = 0.005)和治疗失败均有保护作用(OR 0.29,95% CI 0.13 - 0.66,P = 0.003)。同时使用免疫调节剂治疗也与免疫原性及英夫利昔单抗治疗失败呈负相关(分别为OR 0.31,95% CI 0.15 - 0.65,P = 0.002;OR 0.42,95% CI 0.18 - 0.99,P = 0.04),而间歇性治疗与这两个结局均呈正相关(分别为OR 4.2,95% CI 1.07 - 16.1,P = 0.04;OR 4.45,95% CI 1.2 - 16.6,P = 0.026)。所有其他变量,包括IBD类型、性别、体重、年龄、吸烟状况和病程,均不能预测ATI形成或临床失败。然而,在克罗恩病患者中,非狭窄非穿透性表型对ATI形成有保护作用(OR 0.4,95% CI 0.14 - 0.96,P = 0.04)。犹太阿什肯纳兹族裔对ATI形成和英夫利昔单抗治疗失败具有保护作用。这些发现表明种族因素,以及隐含的遗传易感性,在调节抗TNF免疫原性风险和治疗无反应性方面发挥作用。