Klop C, Gibson-Smith D, Elders P J M, Welsing P M J, Leufkens H G M, Harvey N C, Bijlsma J W J, van Staa T-P, de Vries F
Utrecht Institute for Pharmaceutical Sciences, Division of Pharmacoepidemiology & Clinical Pharmacology, Utrecht University, Universiteitsweg 99, 3584 CG, Utrecht, The Netherlands.
Osteoporos Int. 2015 Jul;26(7):1919-28. doi: 10.1007/s00198-015-3098-x. Epub 2015 May 12.
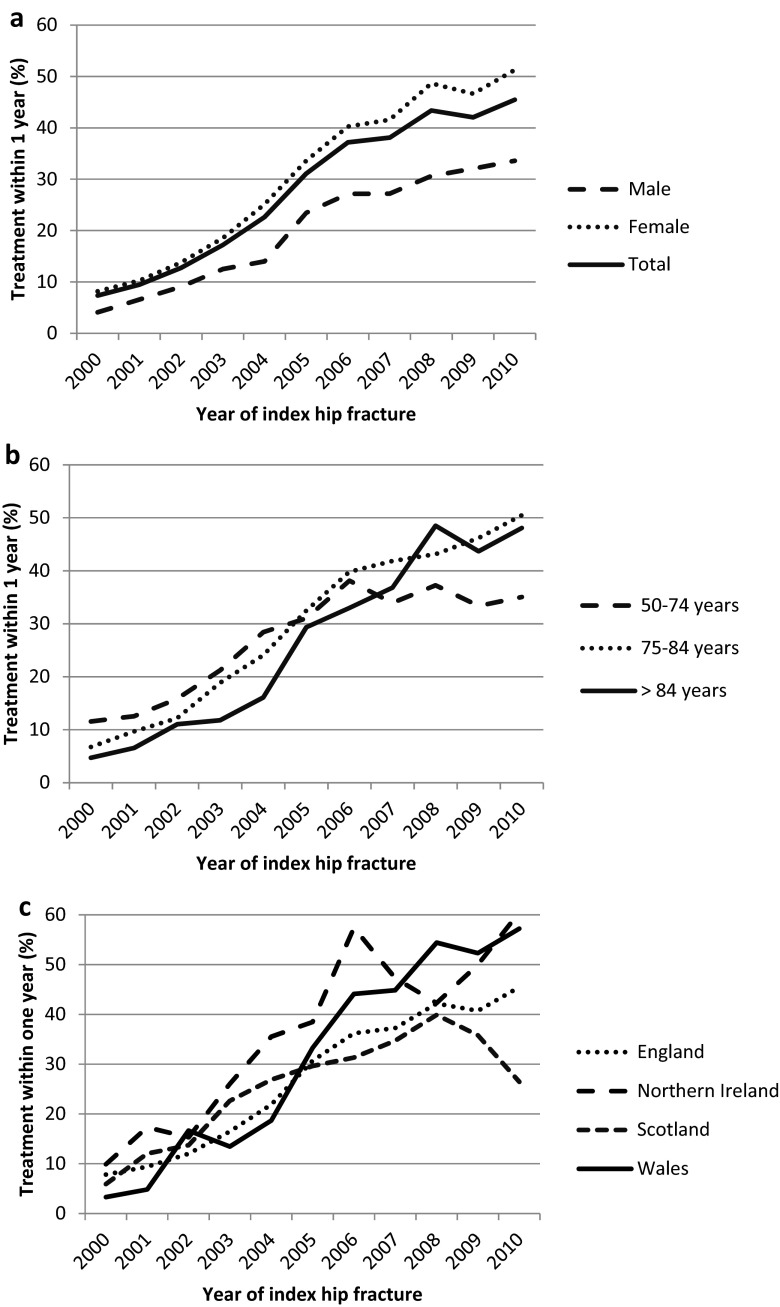
The probability of initiating with anti-osteoporosis therapy increased from 7 % in 2000 to 46 % in 2010. This improvement was greater for patients over the age of 75 years. Men, those overweight, having dementia or exposed to antipsychotics, sedatives/hypnotics or opioid analgesics were significantly less likely to receive anti-osteoporosis drugs.
The objective of this study was to examine trends and determinants of anti-osteoporosis drug prescribing after hip fracture in the UK between 2000 and 2010.
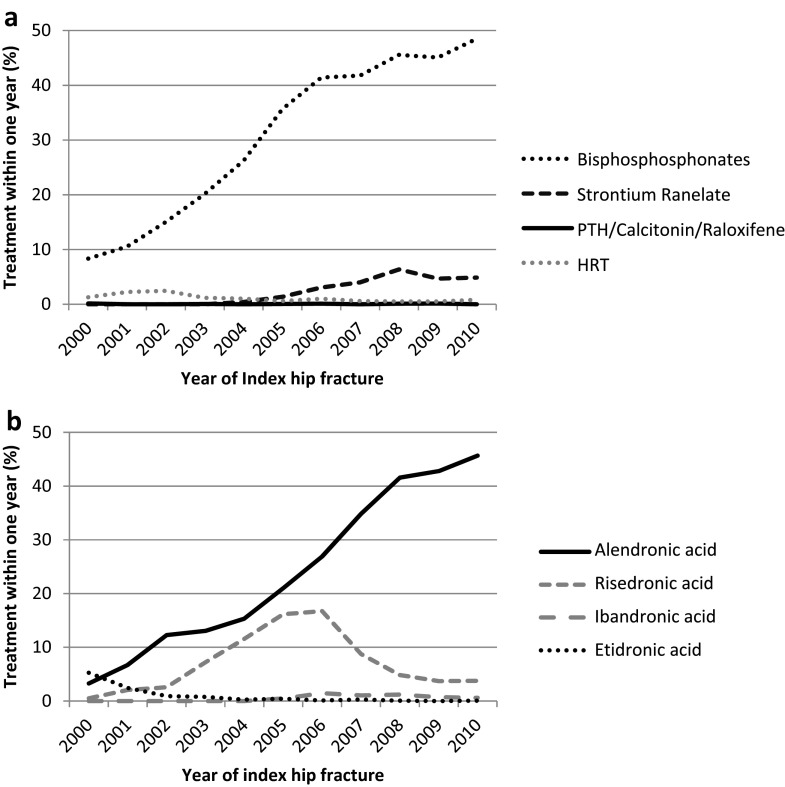
Data were extracted from the UK Clinical Practice Research Datalink for patients ≥50 years who had a first hip fracture between 2000 and 2010 and who did not currently (≤6 months prior) receive anti-osteoporosis drugs (bisphosphonates, strontium ranelate, parathyroid hormone, calcitonin and raloxifene) (n = 27,542). The cumulative incidence probability of being prescribed anti-osteoporosis drugs within 1 year after hip fracture was estimated by Kaplan-Meier life-table analyses. Determinants for treatment initiation were estimated by Cox proportional hazards models.
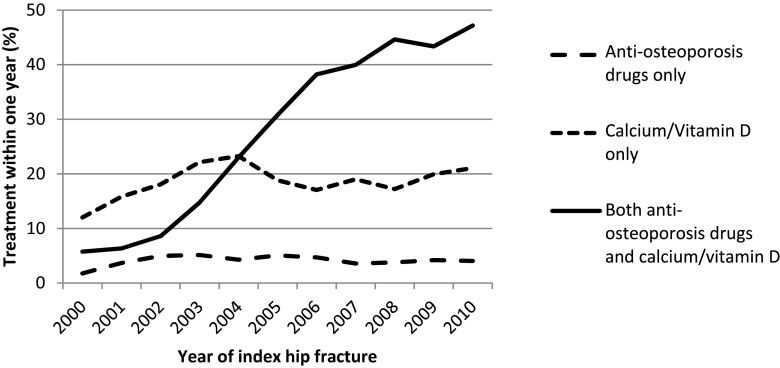
The probability of being prescribed any anti-osteoporosis drug after hip fracture increased from 7 % in 2000 to 46 % in 2010. This trend was more marked in patients ≥75 years. The increase in prescribing of anti-osteoporosis drugs was complemented by a similar increase in vitamin D/calcium provision. Cumulative incidence of receiving anti-osteoporosis therapy was greater at any given point in time in women (8 % in 2000, 51 % in 2010) compared to men (4 % in 2000, 34 % in 2010). In addition to male gender, multivariable Cox regression identified reduced likelihood of receiving anti-osteoporosis drugs for those being overweight, having dementia and exposed to psychotropic drugs (antipsychotics, sedatives/hypnotics) or opioid analgesics.
Although the prescribing of anti-osteoporosis drugs after hip fracture has increased substantially since 2000, the overall rate remained inadequate, particularly in men. With the continuing increase in the absolute number of hip fractures, further research should be made into the barriers to optimise osteoporosis management.
启动抗骨质疏松治疗的概率从2000年的7%升至2010年的46%。75岁以上患者的这一改善更为显著。男性、超重者、患有痴呆症者或使用抗精神病药、镇静剂/催眠药或阿片类镇痛药者接受抗骨质疏松药物治疗的可能性显著降低。
本研究的目的是调查2000年至2010年英国髋部骨折后抗骨质疏松药物处方的趋势和决定因素。
从英国临床实践研究数据链中提取2000年至2010年首次发生髋部骨折且目前(≤6个月前)未接受抗骨质疏松药物(双膦酸盐、雷奈酸锶、甲状旁腺激素、降钙素和雷洛昔芬)治疗的≥50岁患者的数据(n = 27,542)。通过Kaplan-Meier生存表分析估计髋部骨折后1年内开具抗骨质疏松药物的累积发病概率。通过Cox比例风险模型估计治疗启动的决定因素。
髋部骨折后开具任何抗骨质疏松药物的概率从2000年的7%升至2010年的46%。这一趋势在≥75岁的患者中更为明显。抗骨质疏松药物处方量的增加伴随着维生素D/钙供应量的类似增加。在任何给定时间点,女性接受抗骨质疏松治疗的累积发病率(2000年为8%,2010年为51%)高于男性(2000年为4%,2010年为34%)。除了男性性别外,多变量Cox回归分析表明,超重、患有痴呆症以及使用精神药物(抗精神病药、镇静剂/催眠药)或阿片类镇痛药的患者接受抗骨质疏松药物治疗的可能性降低。
尽管自2000年以来髋部骨折后抗骨质疏松药物的处方量大幅增加,但总体比例仍然不足,尤其是在男性中。随着髋部骨折绝对数量的持续增加,应进一步研究优化骨质疏松管理的障碍。