Sierra Saleta, Dybowski J Nikolai, Pironti Alejandro, Heider Dominik, Güney Lisa, Thielen Alex, Reuter Stefan, Esser Stefan, Fätkenheuer Gerd, Lengauer Thomas, Hoffmann Daniel, Pfister Herbert, Jensen Björn, Kaiser Rolf
Institute of Virology, University of Cologne, Cologne, Germany.
Department for Bioinformatics, University of Duisburg-Essen, Essen, Germany.
PLoS One. 2015 May 13;10(5):e0125502. doi: 10.1371/journal.pone.0125502. eCollection 2015.
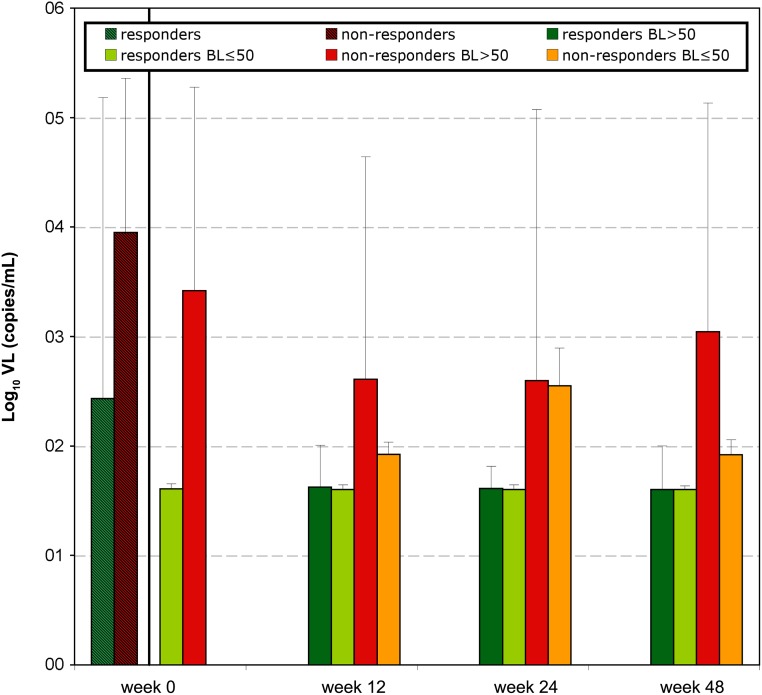
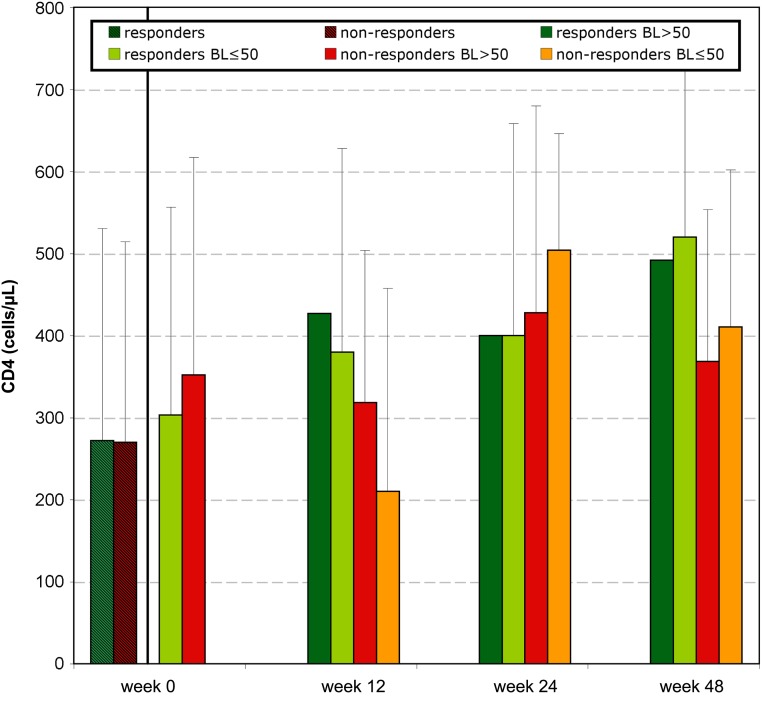
We analysed the impact of different parameters on genotypic tropism testing related to clinical outcome prediction in 108 patients on maraviroc (MVC) treatment.
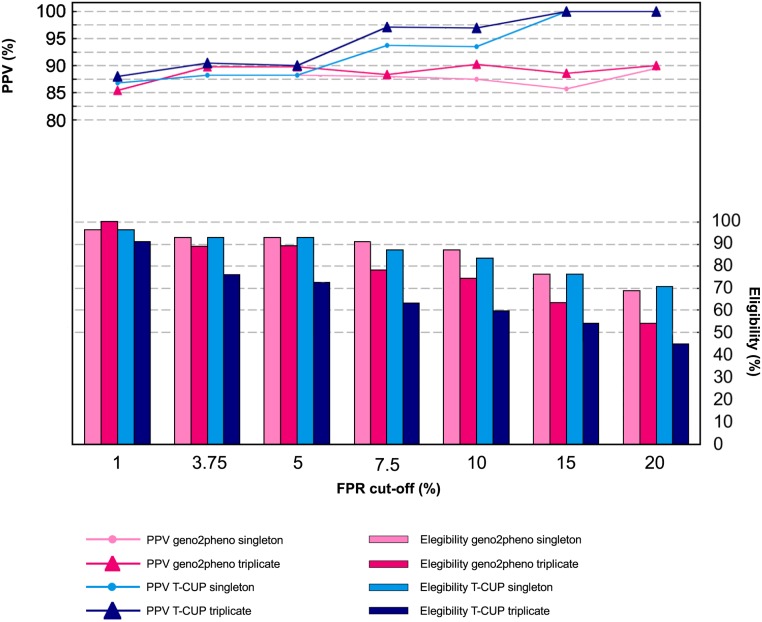
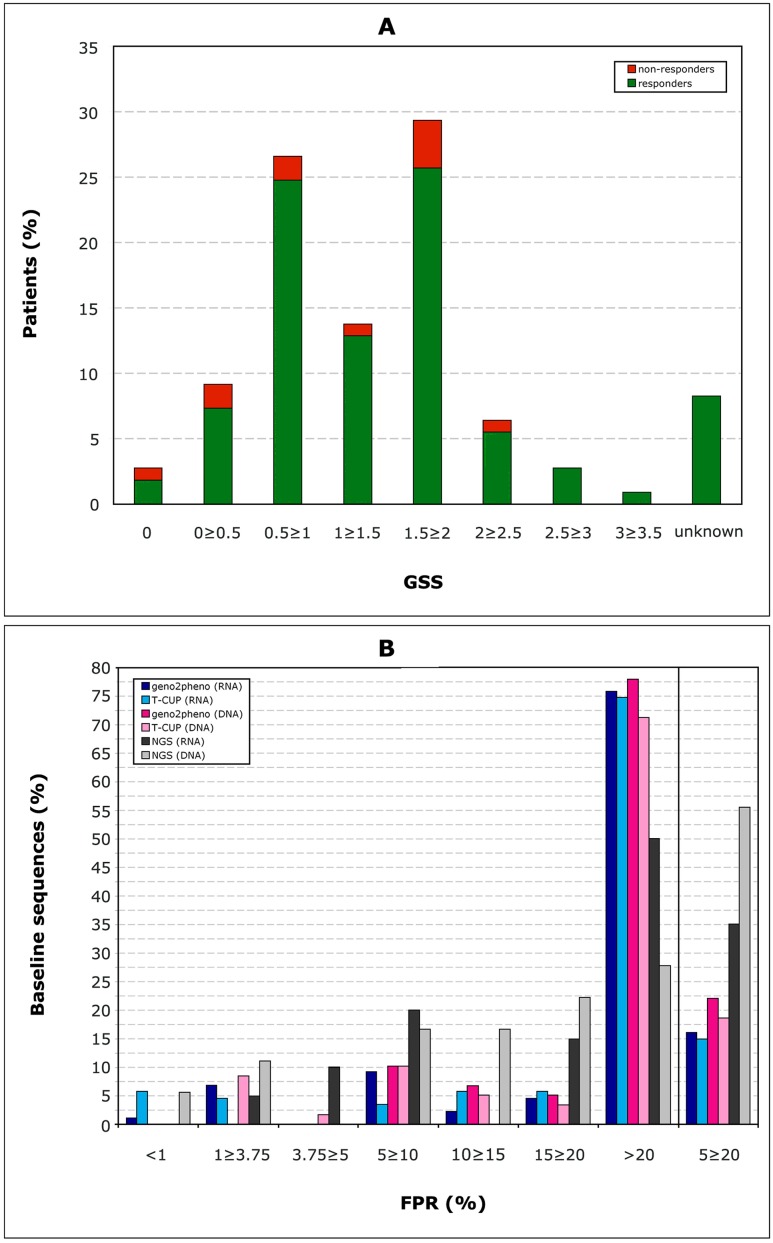
87 RNA and 60 DNA samples were used. The viral tropism was predicted using the geno2pheno[coreceptor] and T-CUP tools with FPR cut-offs ranging from 1%-20%. Additionally, 27 RNA and 28 DNA samples were analysed in triplicate, 43 samples with the ESTA assay and 45 with next-generation sequencing. The influence of the genotypic susceptibility score (GSS) and 16 MVC-resistance mutations on clinical outcome was also studied.
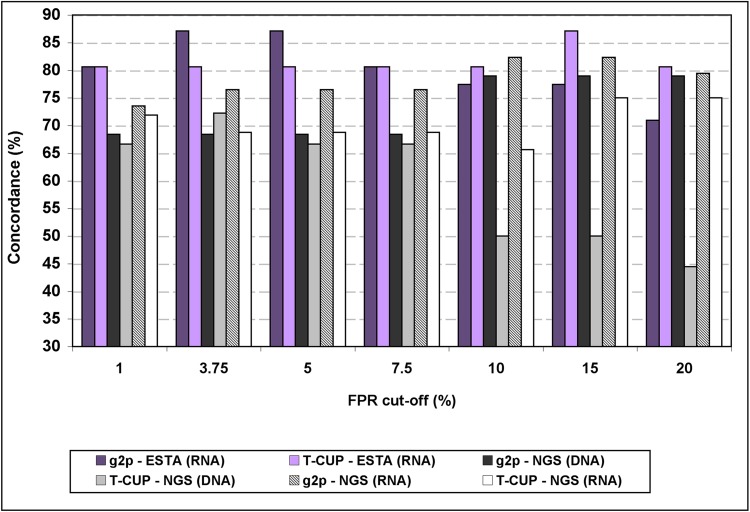
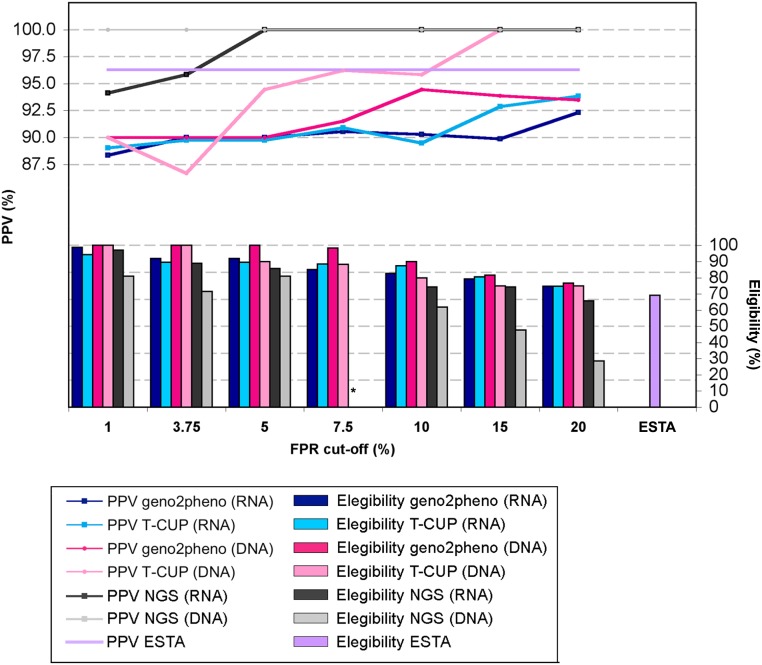
Concordance between single-amplification testing compared to ESTA and to NGS was in the order of 80%. Concordance with NGS was higher at lower FPR cut-offs. Detection of baseline R5 viruses in RNA and DNA samples by all methods significantly correlated with treatment success, even with FPR cut-offs of 3.75%-7.5%. Triple amplification did not improve the prediction value but reduced the number of patients eligible for MVC. No influence of the GSS or MVC-resistance mutations but adherence to treatment, on the clinical outcome was detected.
Proviral DNA is valid to select candidates for MVC treatment. FPR cut-offs of 5%-7.5% and single amplification from RNA or DNA would assure a safe administration of MVC without excluding many patients who could benefit from this drug. In addition, the new prediction system T-CUP produced reliable results.
我们分析了不同参数对108例接受马拉维若(MVC)治疗患者的基因型嗜性检测的影响,该检测与临床结局预测相关。
使用了87份RNA样本和60份DNA样本。使用geno2pheno[共受体]和T-CUP工具预测病毒嗜性,假阳性率(FPR)截止值范围为1%-20%。此外,对27份RNA样本和28份DNA样本进行了三次重复分析,43份样本采用ESTA检测法,45份样本采用下一代测序法。还研究了基因型易感性评分(GSS)和16种MVC耐药突变对临床结局的影响。
单扩增检测与ESTA检测以及与下一代测序检测之间的一致性约为80%。在较低的FPR截止值下,与下一代测序的一致性更高。所有方法在RNA和DNA样本中检测到基线R5病毒均与治疗成功显著相关,即使FPR截止值为3.75%-7.5%。三次扩增并未提高预测价值,但减少了符合MVC治疗条件的患者数量。未检测到GSS或MVC耐药突变对临床结局有影响,但检测到治疗依从性对临床结局有影响。
前病毒DNA对于选择MVC治疗候选者是有效的。5%-7.5%的FPR截止值以及从RNA或DNA进行单扩增将确保安全使用MVC,而不会排除许多可能从该药物中获益的患者。此外,新的预测系统T-CUP产生了可靠的结果。