Barbagallo Simone, Corradi Luca, de Ville de Goyet Jean, Iannucci Marina, Porro Ivan, Rosso Nicola, Tanfani Elena, Testi Angela
Bambino Gesù Children's Hospital, Piazza San Onofrio 4, Rome, 00165, Italy.
Nextage s.r.l, Genoa, Italy.
BMC Med Inform Decis Mak. 2015 May 17;15:38. doi: 10.1186/s12911-015-0161-7.
The Operating Room (OR) is a key resource of all major hospitals, but it also accounts for up 40% of resource costs. Improving cost effectiveness, while maintaining a quality of care, is a universal objective. These goals imply an optimization of planning and a scheduling of the activities involved. This is highly challenging due to the inherent variable and unpredictable nature of surgery.
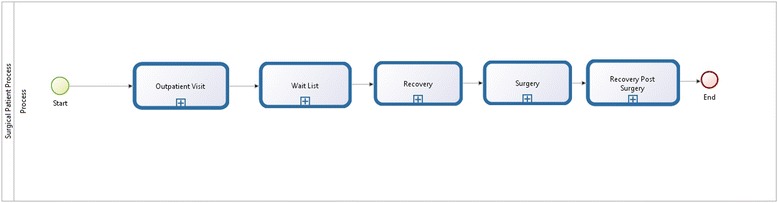
A Business Process Modeling Notation (BPMN 2.0) was used for the representation of the "OR Process" (being defined as the sequence of all of the elementary steps between "patient ready for surgery" to "patient operated upon") as a general pathway ("path"). The path was then both further standardized as much as possible and, at the same time, keeping all of the key-elements that would allow one to address or define the other steps of planning, and the inherent and wide variability in terms of patient specificity. The path was used to schedule OR activity, room-by-room, and day-by-day, feeding the process from a "waiting list database" and using a mathematical optimization model with the objective of ending up in an optimized planning.
The OR process was defined with special attention paid to flows, timing and resource involvement. Standardization involved a dynamics operation and defined an expected operating time for each operation. The optimization model has been implemented and tested on real clinical data. The comparison of the results reported with the real data, shows that by using the optimization model, allows for the scheduling of about 30% more patients than in actual practice, as well as to better exploit the OR efficiency, increasing the average operating room utilization rate up to 20%.
The optimization of OR activity planning is essential in order to manage the hospital's waiting list. Optimal planning is facilitated by defining the operation as a standard pathway where all variables are taken into account. By allowing a precise scheduling, it feeds the process of planning and, further up-stream, the management of a waiting list in an interactive and bi-directional dynamic process.
手术室是所有大型医院的关键资源,但它也占资源成本的40%。在保持医疗质量的同时提高成本效益是一个普遍目标。这些目标意味着要优化规划和安排相关活动。由于手术本身具有多变性和不可预测性,这极具挑战性。
使用业务流程建模符号(BPMN 2.0)将“手术室流程”(定义为从“患者准备手术”到“患者手术完成”之间所有基本步骤的序列)表示为一条通用路径(“路径”)。然后尽可能进一步规范该路径,同时保留所有关键要素,这些要素将有助于处理或定义规划的其他步骤,以及患者特异性方面固有的广泛变异性。该路径用于逐间手术室、逐日安排手术室活动,从“候诊名单数据库”输入流程,并使用数学优化模型,目标是实现优化规划。
定义手术室流程时特别关注流程、时间安排和资源投入。标准化涉及动态操作,并为每个手术定义了预期手术时间。该优化模型已在实际临床数据上实施和测试。将报告结果与实际数据进行比较,结果表明,使用优化模型比实际操作可多安排约30%的患者,还能更好地利用手术室效率,将平均手术室利用率提高到20%。
优化手术室活动规划对于管理医院候诊名单至关重要。通过将手术定义为考虑所有变量的标准路径,有助于实现最佳规划。通过实现精确的调度,它为规划流程提供支持,并在更上游的层面,以交互式和双向动态流程管理候诊名单。