Dulai Parambir S, Levesque Barrett G, Feagan Brian G, D'Haens Geert, Sandborn William J
University of California San Diego, San Diego, California; Robarts Clinical Trials, Robarts Research Institute, Western University, London, Ontario, Canada.
Robarts Clinical Trials, Robarts Research Institute, Western University, London, Ontario, Canada; Department of Medicine, Western University, London, Ontario, Canada.
Gastrointest Endosc. 2015 Aug;82(2):246-55. doi: 10.1016/j.gie.2015.03.1974. Epub 2015 May 21.
Mucosal healing is an important treatment end-point in inflammatory bowel disease, and achieving mucosal healing has been demonstrated to improve disease-related outcomes. Considerable uncertainty exists, however, regarding the optimal approach for the assessment of mucosal healing.
To compare currently available diagnostic tools for the assessment of mucosal healing and outline the ideal approach to integrating these tools into clinical trials and clinical practice.
Review article.
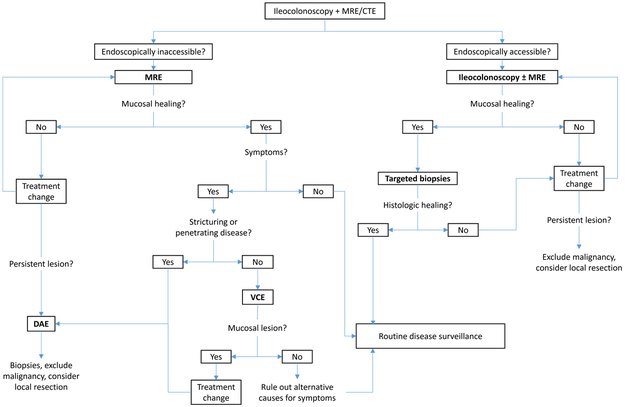
Endoscopy represents the criterion standard for the assessment of mucosal healing, and frequent endoscopic assessment is associated with a higher rate of achieving mucosal healing. The use of mucosal biopsy allows for the identification of persistent histologic disease activity, but the incremental clinical benefit of achieving histologic healing is yet to be determined. Magnetic resonance enterography has a high sensitivity for ulcer healing in endoscopically inaccessible disease activity. However, the presence of mucosal lesions cannot be reliably excluded based on this modality alone, and further small-bowel endoscopy should be considered in symptomatic patients. Video capsule endoscopy or device-assisted enteroscopy can be used, with device-assisted enteroscopy being preferred in stricturing Crohn's disease because of the risk of capsule retention or in patients in whom small-bowel malignancy is a possibility.
Endoscopy remains the criterion standard for the assessment of mucosal healing. Several alternative diagnostic modalities have become available that can be of value in specific clinical circumstances, particularly in patients with small-bowel involvement.
黏膜愈合是炎症性肠病重要的治疗终点,且已证实实现黏膜愈合可改善疾病相关结局。然而,关于评估黏膜愈合的最佳方法仍存在相当大的不确定性。
比较目前用于评估黏膜愈合的诊断工具,并概述将这些工具整合到临床试验和临床实践中的理想方法。
综述文章。
内镜检查是评估黏膜愈合的标准方法,频繁的内镜评估与实现黏膜愈合的更高发生率相关。黏膜活检可用于识别持续性组织学疾病活动,但实现组织学愈合的额外临床益处尚待确定。磁共振小肠造影对内镜难以到达的疾病活动中的溃疡愈合具有高敏感性。然而,仅基于这种检查方式不能可靠地排除黏膜病变的存在,对于有症状的患者应考虑进一步行小肠内镜检查。可使用视频胶囊内镜或器械辅助小肠镜检查,在狭窄性克罗恩病中,由于存在胶囊滞留风险或在可能患有小肠恶性肿瘤的患者中,器械辅助小肠镜检查更受青睐。
内镜检查仍然是评估黏膜愈合的标准方法。已有几种替代诊断方法,它们在特定临床情况下可能有价值,特别是在小肠受累的患者中。