Wiegman Albert, Gidding Samuel S, Watts Gerald F, Chapman M John, Ginsberg Henry N, Cuchel Marina, Ose Leiv, Averna Maurizio, Boileau Catherine, Borén Jan, Bruckert Eric, Catapano Alberico L, Defesche Joep C, Descamps Olivier S, Hegele Robert A, Hovingh G Kees, Humphries Steve E, Kovanen Petri T, Kuivenhoven Jan Albert, Masana Luis, Nordestgaard Børge G, Pajukanta Päivi, Parhofer Klaus G, Raal Frederick J, Ray Kausik K, Santos Raul D, Stalenhoef Anton F H, Steinhagen-Thiessen Elisabeth, Stroes Erik S, Taskinen Marja-Riitta, Tybjærg-Hansen Anne, Wiklund Olov
Department of Paediatrics, Academic Medical Center, University of Amsterdam, The Netherlands
Nemours Cardiac Center, A. I. DuPont Hospital for Children, Wilmington, DE, USA.
Eur Heart J. 2015 Sep 21;36(36):2425-37. doi: 10.1093/eurheartj/ehv157. Epub 2015 May 25.
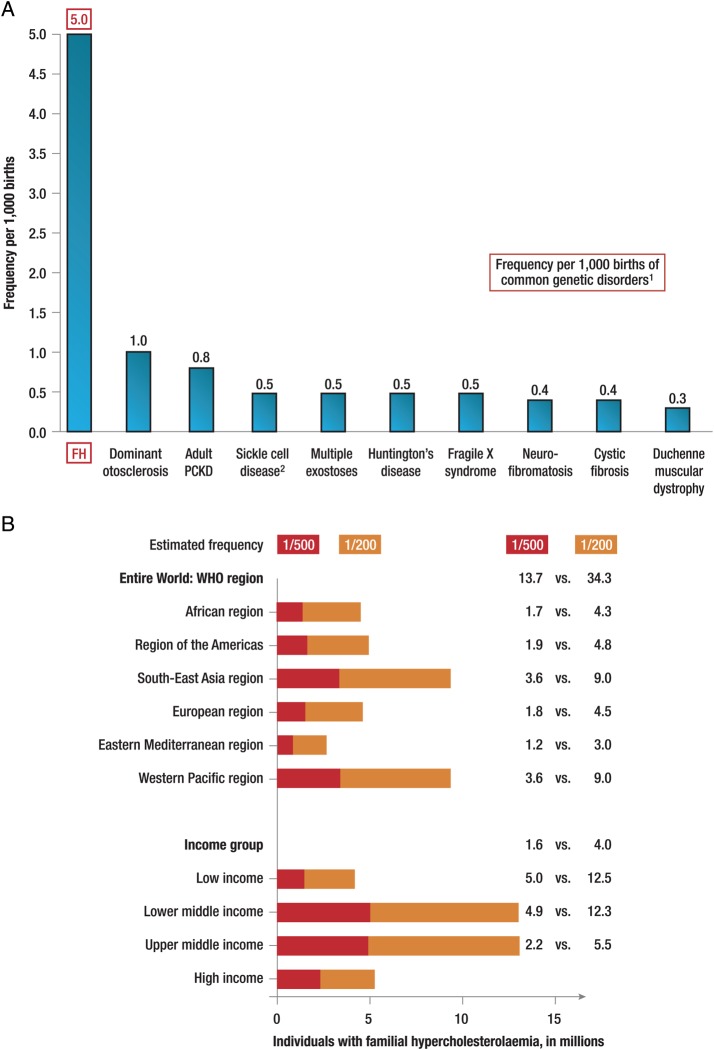
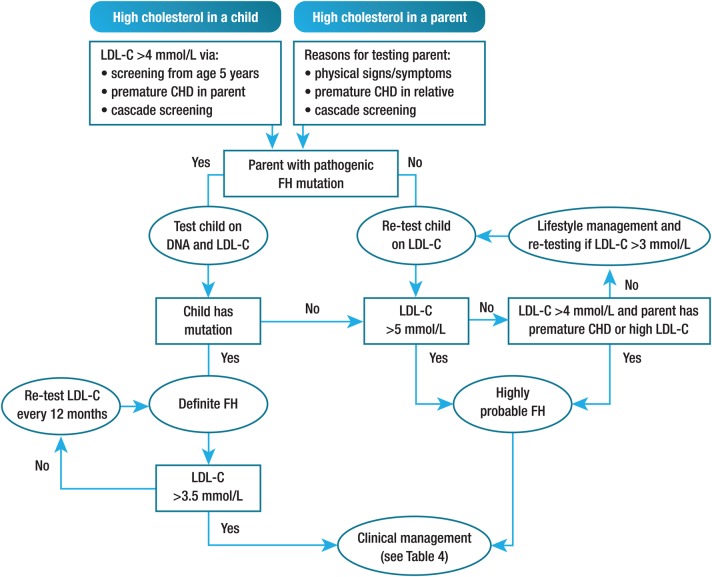
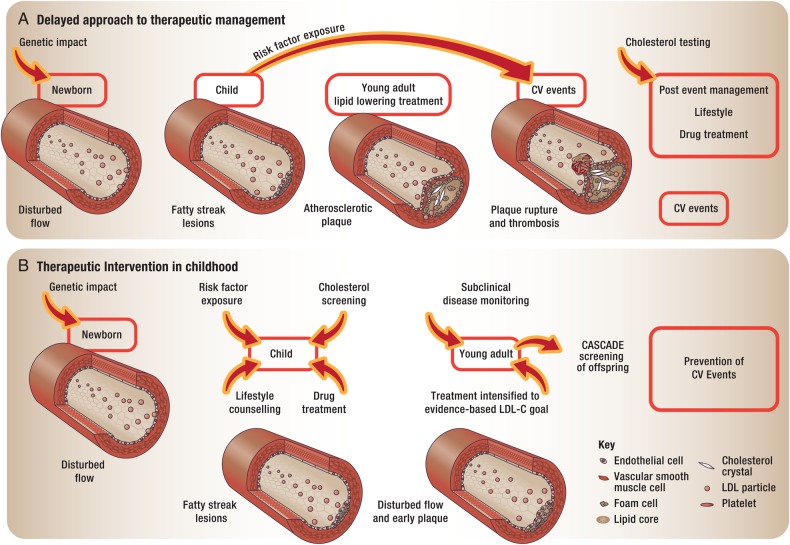
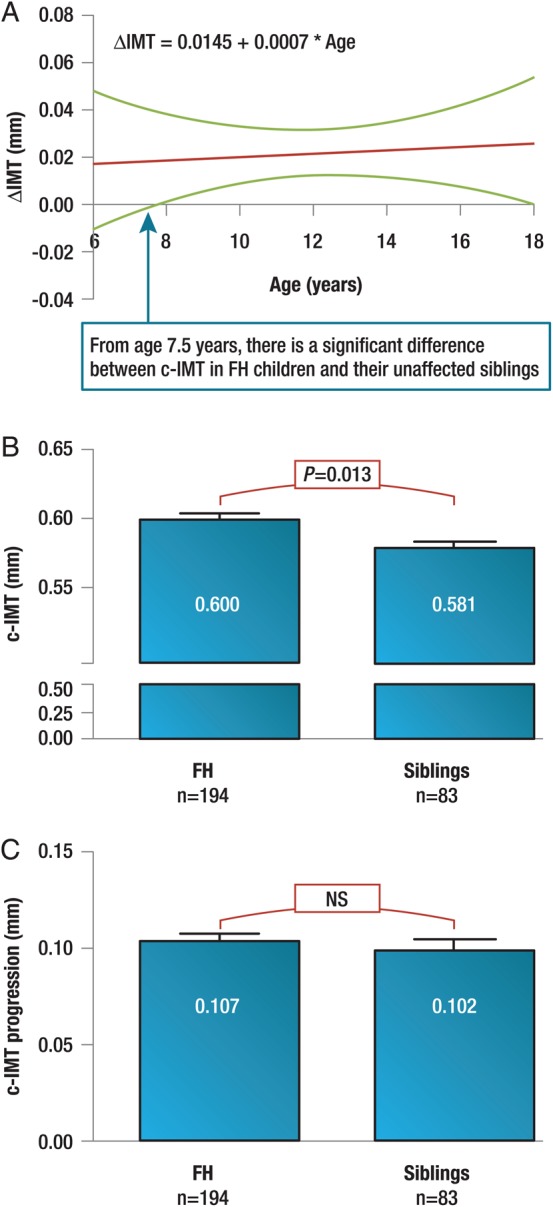
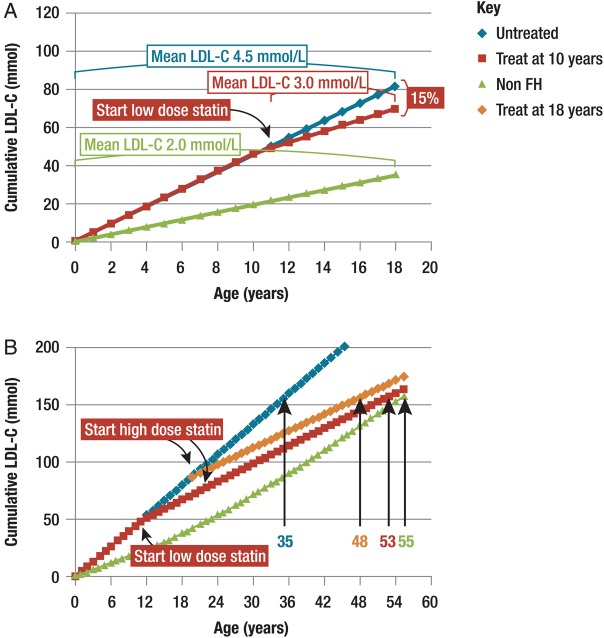
Familial hypercholesterolaemia (FH) is a common genetic cause of premature coronary heart disease (CHD). Globally, one baby is born with FH every minute. If diagnosed and treated early in childhood, individuals with FH can have normal life expectancy. This consensus paper aims to improve awareness of the need for early detection and management of FH children. Familial hypercholesterolaemia is diagnosed either on phenotypic criteria, i.e. an elevated low-density lipoprotein cholesterol (LDL-C) level plus a family history of elevated LDL-C, premature coronary artery disease and/or genetic diagnosis, or positive genetic testing. Childhood is the optimal period for discrimination between FH and non-FH using LDL-C screening. An LDL-C ≥5 mmol/L (190 mg/dL), or an LDL-C ≥4 mmol/L (160 mg/dL) with family history of premature CHD and/or high baseline cholesterol in one parent, make the phenotypic diagnosis. If a parent has a genetic defect, the LDL-C cut-off for the child is ≥3.5 mmol/L (130 mg/dL). We recommend cascade screening of families using a combined phenotypic and genotypic strategy. In children, testing is recommended from age 5 years, or earlier if homozygous FH is suspected. A healthy lifestyle and statin treatment (from age 8 to 10 years) are the cornerstones of management of heterozygous FH. Target LDL-C is <3.5 mmol/L (130 mg/dL) if >10 years, or ideally 50% reduction from baseline if 8-10 years, especially with very high LDL-C, elevated lipoprotein(a), a family history of premature CHD or other cardiovascular risk factors, balanced against the long-term risk of treatment side effects. Identifying FH early and optimally lowering LDL-C over the lifespan reduces cumulative LDL-C burden and offers health and socioeconomic benefits. To drive policy change for timely detection and management, we call for further studies in the young. Increased awareness, early identification, and optimal treatment from childhood are critical to adding decades of healthy life for children and adolescents with FH.
家族性高胆固醇血症(FH)是早发性冠心病(CHD)的常见遗传病因。在全球范围内,每分钟就有一名患有FH的婴儿出生。如果在儿童期能够早期诊断并接受治疗,FH患者的预期寿命可以正常。本共识文件旨在提高对早期发现和管理FH儿童必要性的认识。家族性高胆固醇血症可根据表型标准进行诊断,即低密度脂蛋白胆固醇(LDL-C)水平升高加上LDL-C升高、早发性冠状动脉疾病和/或遗传诊断的家族史,或基因检测呈阳性。儿童期是使用LDL-C筛查区分FH和非FH的最佳时期。LDL-C≥5 mmol/L(190 mg/dL),或LDL-C≥4 mmol/L(160 mg/dL)且有早发性冠心病家族史和/或父母一方基线胆固醇水平高,则可做出表型诊断。如果父母有基因缺陷,儿童的LDL-C临界值为≥3.5 mmol/L(130 mg/dL)。我们建议采用表型和基因型相结合的策略对家族进行级联筛查。对于儿童,建议从5岁开始进行检测,如果怀疑是纯合子FH则更早进行检测。健康的生活方式和他汀类药物治疗(8至10岁开始)是杂合子FH管理的基石。如果年龄>10岁,目标LDL-C<3.5 mmol/L(130 mg/dL),如果年龄在8 - 10岁,理想情况是从基线降低50%,特别是对于LDL-C非常高、脂蛋白(a)升高、有早发性冠心病家族史或其他心血管危险因素的情况,同时要权衡治疗副作用的长期风险。在整个生命周期中早期识别FH并最佳地降低LDL-C可减少累积的LDL-C负担,并带来健康和社会经济效益。为推动政策变革以实现及时检测和管理,我们呼吁对年轻人进行进一步研究。提高认识、早期识别以及从儿童期开始进行最佳治疗对于为患有FH的儿童和青少年增加数十年健康生活至关重要。