Huo Cecilia W, Chew Grace, Hill Prue, Huang Dexing, Ingman Wendy, Hodson Leigh, Brown Kristy A, Magenau Astrid, Allam Amr H, McGhee Ewan, Timpson Paul, Henderson Michael A, Thompson Erik W, Britt Kara
University of Melbourne Department of Surgery, St. Vincent's Hospital, Level 2, Clinical Sciences Building, 29 Regent Street, Fitzroy, VIC, 3065, Australia.
Department of Pathology, St. Vincent's Hospital, 41 Victoria Parade, Fitzroy, VIC, 3065, Australia.
Breast Cancer Res. 2015 Jun 4;17(1):79. doi: 10.1186/s13058-015-0592-1.
Mammographic density (MD), after adjustment for a women's age and body mass index, is a strong and independent risk factor for breast cancer (BC). Although the BC risk attributable to increased MD is significant in healthy women, the biological basis of high mammographic density (HMD) causation and how it raises BC risk remain elusive. We assessed the histological and immunohistochemical differences between matched HMD and low mammographic density (LMD) breast tissues from healthy women to define which cell features may mediate the increased MD and MD-associated BC risk.
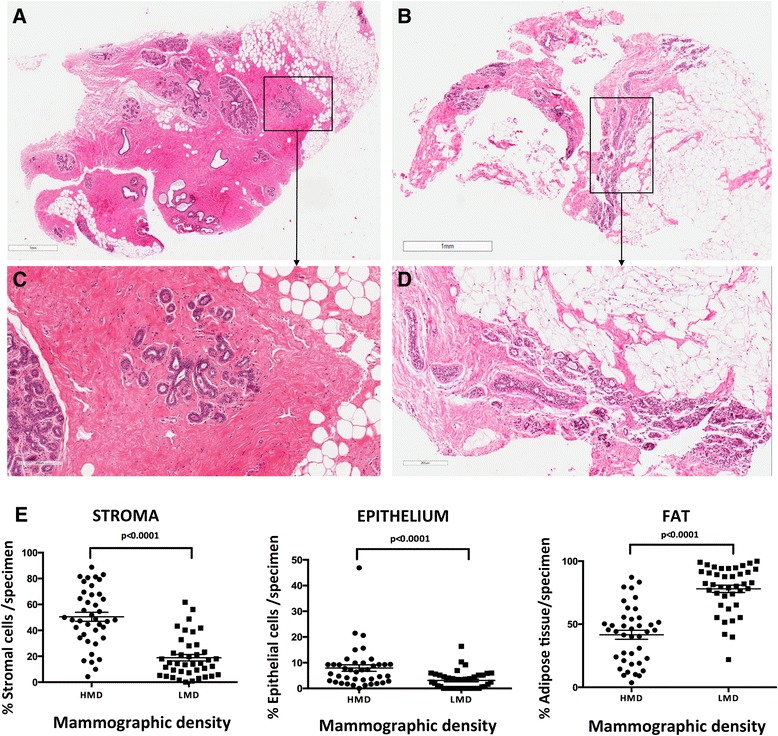
Tissues were obtained between 2008 and 2013 from 41 women undergoing prophylactic mastectomy because of their high BC risk profile. Tissue slices resected from the mastectomy specimens were X-rayed, then HMD and LMD regions were dissected based on radiological appearance. The histological composition, aromatase immunoreactivity, hormone receptor status and proliferation status were assessed, as were collagen amount and orientation, epithelial subsets and immune cell status.
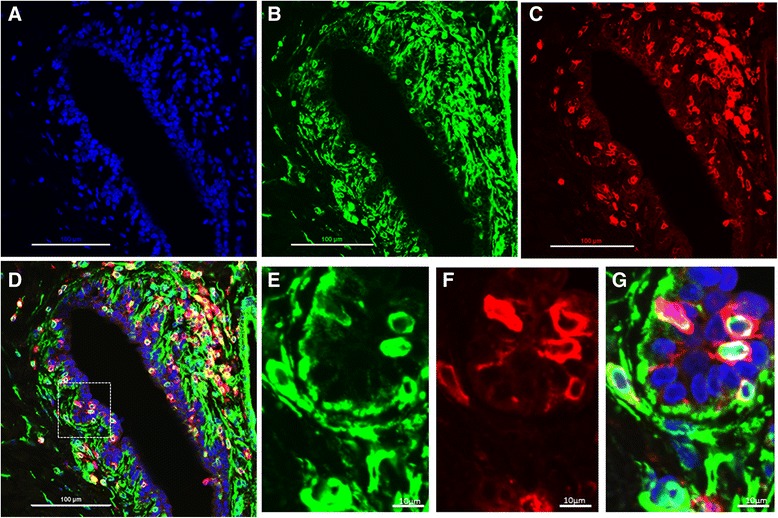
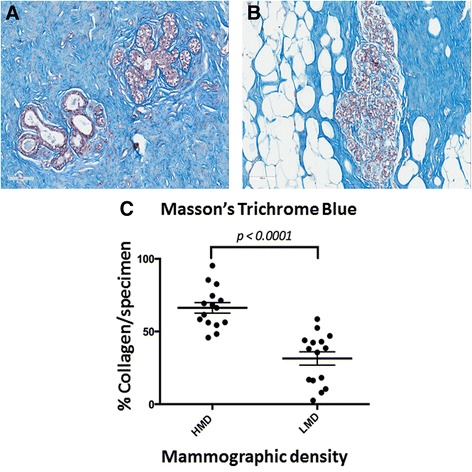
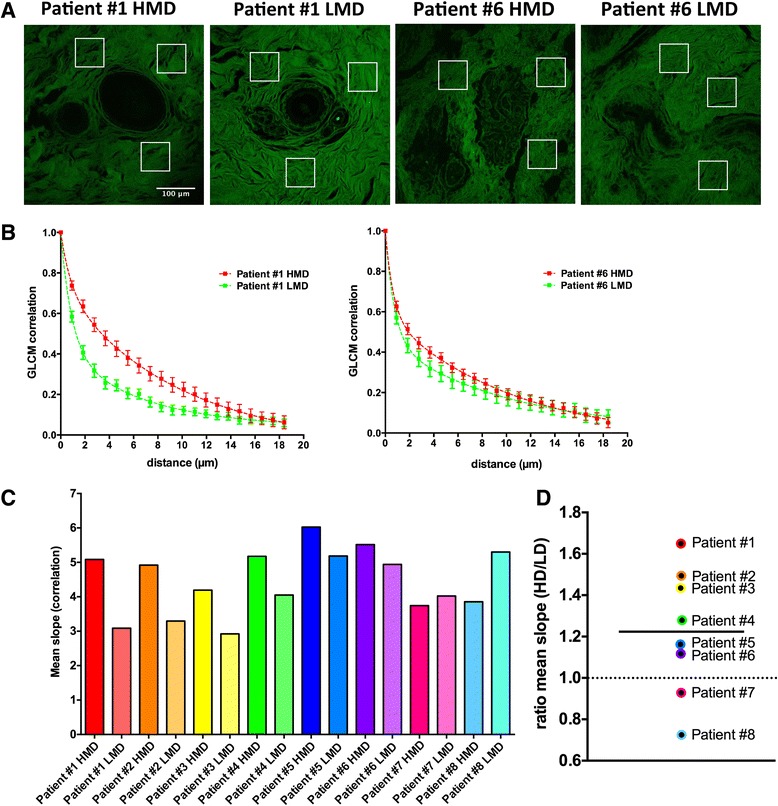
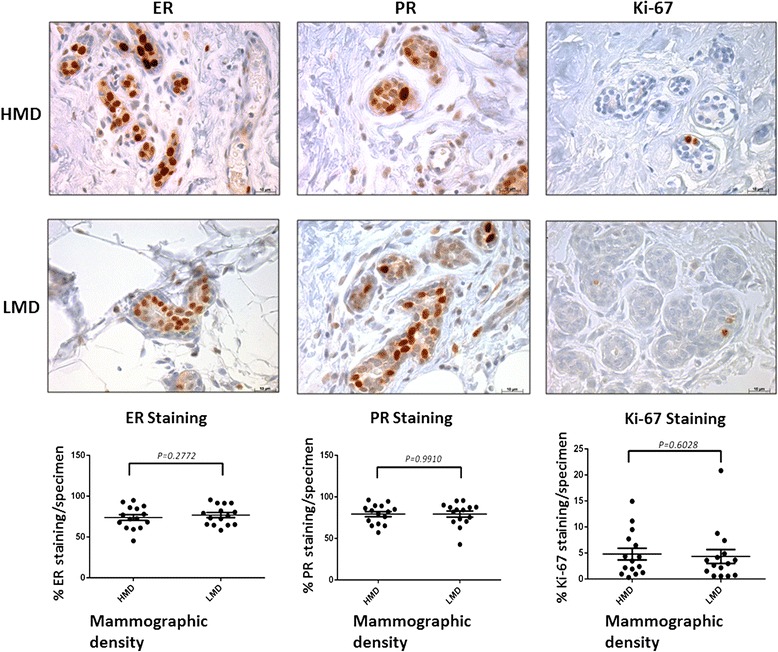
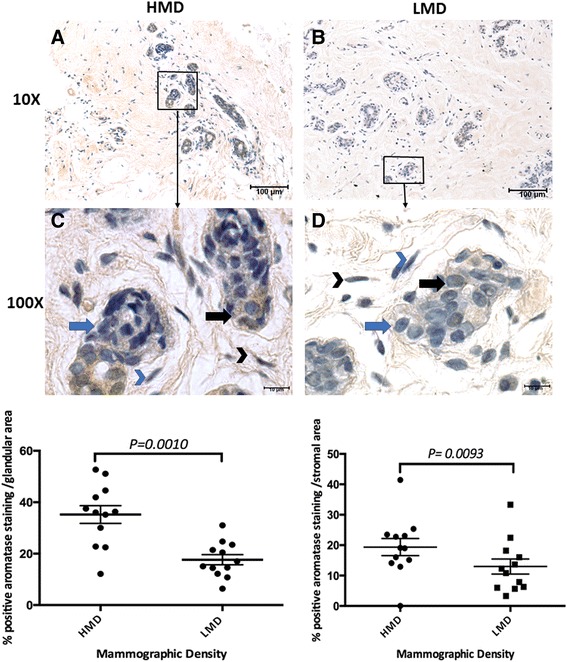
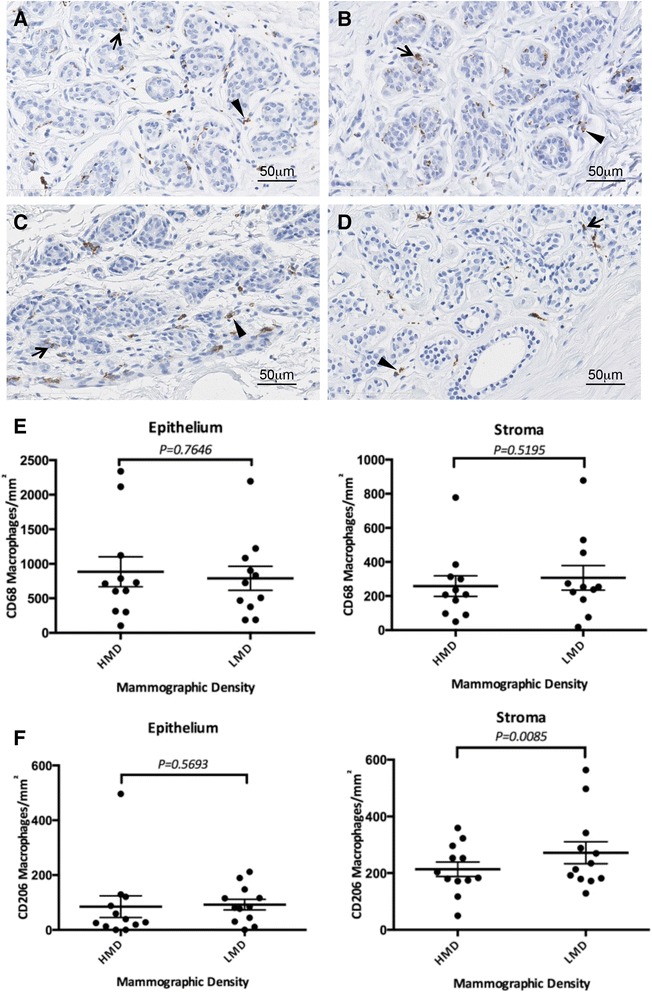
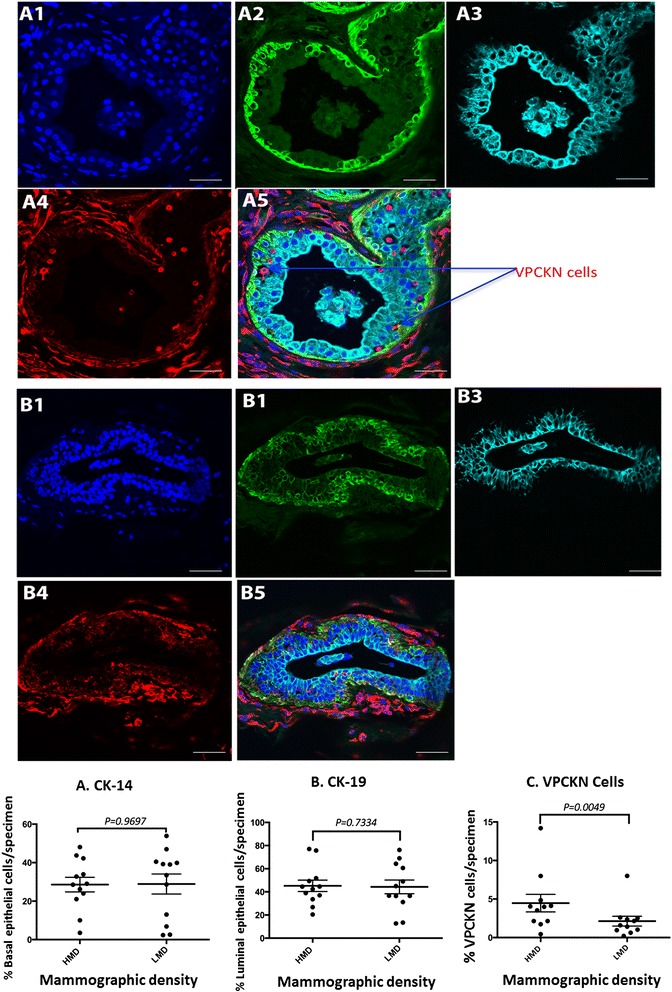
HMD tissue had a significantly greater proportion of stroma, collagen and epithelium, as well as less fat, than LMD tissue did. Second harmonic generation imaging demonstrated more organised stromal collagen in HMD tissues than in LMD tissues. There was significantly more aromatase immunoreactivity in both the stromal and glandular regions of HMD tissues than in those regions of LMD tissues, although no significant differences in levels of oestrogen receptor, progesterone receptor or Ki-67 expression were detected. The number of macrophages within the epithelium or stroma did not change; however, HMD stroma exhibited less CD206(+) alternatively activated macrophages. Epithelial cell maturation was not altered in HMD samples, and no evidence of epithelial-mesenchymal transition was seen; however, there was a significant increase in vimentin(+)/CD45(+) immune cells within the epithelial layer in HMD tissues.
We confirmed increased proportions of stroma and epithelium, increased aromatase activity and no changes in hormone receptor or Ki-67 marker status in HMD tissue. The HMD region showed increased collagen deposition and organisation as well as decreased alternatively activated macrophages in the stroma. The HMD epithelium may be a site for local inflammation, as we observed a significant increase in CD45(+)/vimentin(+) immune cells in this area.
在对女性年龄和体重指数进行调整后,乳腺X线密度(MD)是乳腺癌(BC)的一个强有力的独立风险因素。尽管在健康女性中,因乳腺X线密度增加导致的乳腺癌风险显著,但高乳腺X线密度(HMD)的生物学成因及其如何增加乳腺癌风险仍不清楚。我们评估了健康女性中匹配的高乳腺X线密度和低乳腺X线密度(LMD)乳腺组织之间的组织学和免疫组化差异,以确定哪些细胞特征可能介导乳腺X线密度增加及与乳腺X线密度相关的乳腺癌风险。
2008年至2013年间,从41名因乳腺癌高风险而接受预防性乳房切除术的女性身上获取组织。从乳房切除标本中切取的组织切片进行X线检查,然后根据放射学表现分离出高乳腺X线密度和低乳腺X线密度区域。评估组织学组成、芳香化酶免疫反应性、激素受体状态和增殖状态,以及胶原含量和方向、上皮亚群和免疫细胞状态。
与低乳腺X线密度组织相比,高乳腺X线密度组织的基质、胶原和上皮比例显著更高,脂肪更少。二次谐波产生成像显示,高乳腺X线密度组织中的基质胶原比低乳腺X线密度组织中的更有组织性。高乳腺X线密度组织的基质和腺区域中的芳香化酶免疫反应性明显高于低乳腺X线密度组织的相应区域,尽管未检测到雌激素受体、孕激素受体或Ki-67表达水平的显著差异。上皮或基质内巨噬细胞的数量没有变化;然而,高乳腺X线密度基质中CD206(+)交替激活的巨噬细胞较少。高乳腺X线密度样本中的上皮细胞成熟未改变,也未发现上皮-间质转化的证据;然而,高乳腺X线密度组织的上皮层内波形蛋白(+)/CD45(+)免疫细胞显著增加。
我们证实高乳腺X线密度组织中基质和上皮比例增加、芳香化酶活性增加,激素受体或Ki-67标记物状态无变化。高乳腺X线密度区域显示胶原沉积和组织增加,基质中交替激活的巨噬细胞减少。高乳腺X线密度上皮可能是局部炎症的部位,因为我们在该区域观察到CD45(+)/波形蛋白(+)免疫细胞显著增加。