Gussgard Anne Margrete, Jokstad Asbjorn, Wood Robert, Hope Andrew J, Tenenbaum Howard
Princess Margaret Cancer Centre, Toronto, Ontario, Canada.
Faculty of Dentistry, University of Toronto, Toronto, Ontario, Canada.
PLoS One. 2015 Jun 10;10(6):e0129001. doi: 10.1371/journal.pone.0129001. eCollection 2015.
Self-reported pain and impairment of oral functions varies markedly and often in spite of extensive oral mucositis (OM). The aim of the current study was to appraise how patient-reported debilitation caused by OM is influenced by the extent and possibly location of the OM lesions.
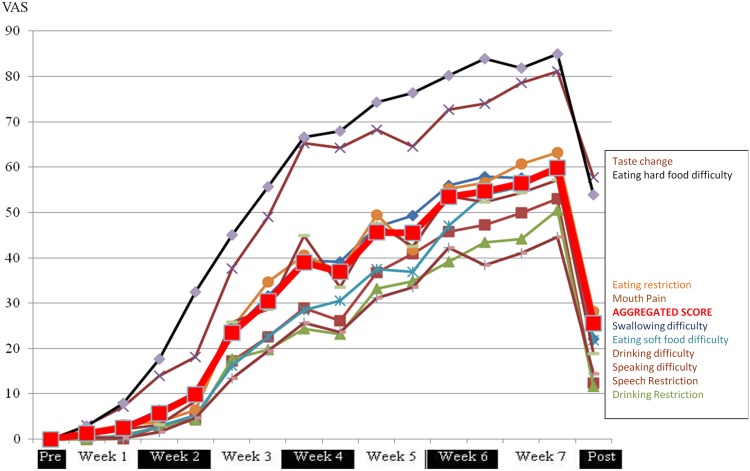
Patients with head and neck cancer undergoing radiotherapy were examined before treatment, twice weekly during 6-7 weeks of therapy, and 3-4 weeks after therapy completion. OM signs of 33 participants were evaluated using the Oral Mucositis Assessment Scale (OMAS), while OM symptoms were recorded using Patient-Reported Oral Mucositis Symptom (PROMS)-questionnaires. Changes in OM experience as a function of OM signs was undertaken by comparing the aggregated and individual PROMS scale values at the point of transition of OMAS ulceration scores between 0 to 1, 1 to 2 and 2 to 3, respectively in the nine intra-oral locations designated in the OMAS. ANOVA with pairwise contrasts using the LSD procedure was applied for comparisons of mean changes of PROMS scale values for the participants who experienced an OMAS score of 2 or more during therapy (n=24).
Impairment of eating hard foods was more when the OMAS score for ulceration anywhere in the mouth or in the soft palate changed from 1 to 2, compared to between score 0 and 1 (p=.002 and p=.05) or between score 2 and 3 (p=.001 and p=.02). Mouth pain increased more upon transition of OMAS score anywhere in the mouth from 1 to 2 compared to 0 to 1 (p=.05).
The relationship between patient-reported impairment of oral function and pain caused by OM ulceration is not linear, but rather curvilinear. Our findings should prompt investigators of future interventional trials to consider using a less severe outcome than maximum OM scores as the primary study outcome.
尽管存在广泛的口腔黏膜炎(OM),但自我报告的疼痛和口腔功能障碍仍有显著差异,且情况各异。本研究的目的是评估OM病变的程度以及可能的位置如何影响患者报告的由OM引起的衰弱。
对头颈部癌放疗患者在治疗前、治疗6 - 7周期间每周两次以及治疗完成后3 - 4周进行检查。使用口腔黏膜炎评估量表(OMAS)评估33名参与者的OM体征,同时使用患者报告的口腔黏膜炎症状(PROMS)问卷记录OM症状。通过比较OMAS溃疡评分在0至1、1至2和2至3之间转换时,在OMAS指定的九个口腔内位置分别汇总和个体的PROMS量表值,来研究OM体验随OM体征的变化。对于治疗期间OMAS评分达到2或更高的参与者(n = 24),采用LSD程序进行成对对比的方差分析,以比较PROMS量表值的平均变化。
与溃疡评分从0到1(p = 0.002和p = 0.05)或从2到3(p = 0.001和p = 0.02)相比,当口腔内任何部位或软腭的溃疡OMAS评分从1变为2时,食用硬食物的障碍更大。与从0到1相比,口腔内任何部位的OMAS评分从1变为2时,口腔疼痛增加更多(p = 0.05)。
患者报告的OM溃疡引起的口腔功能障碍与疼痛之间的关系不是线性的,而是曲线的。我们的研究结果应促使未来干预试验的研究者考虑使用比最大OM评分较轻的结果作为主要研究结果。