Tamaki Tomoaki, Ohno Tatsuya, Noda Shin-ei, Kato Shingo, Nakano Takashi
Department of Radiation Oncology, Saitama Medical University International Medical Center, 1397-1 Yamane, Hidaka, Saitama 350-1298, Japan
Department of Radiation Oncology, Gunma University Graduate School of Medicine, 3-39-22 Showa-machi, Maebashi, Gunma 371-8511 Japan.
J Radiat Res. 2015 Sep;56(5):804-10. doi: 10.1093/jrr/rrv029. Epub 2015 Jun 10.
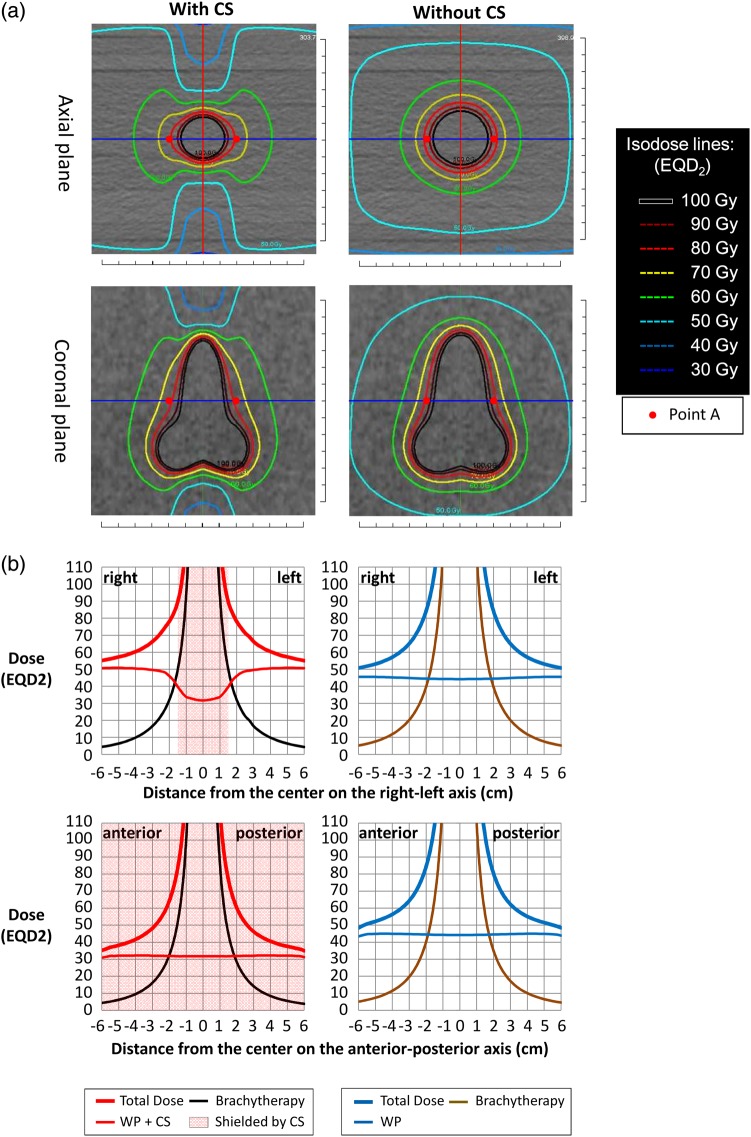
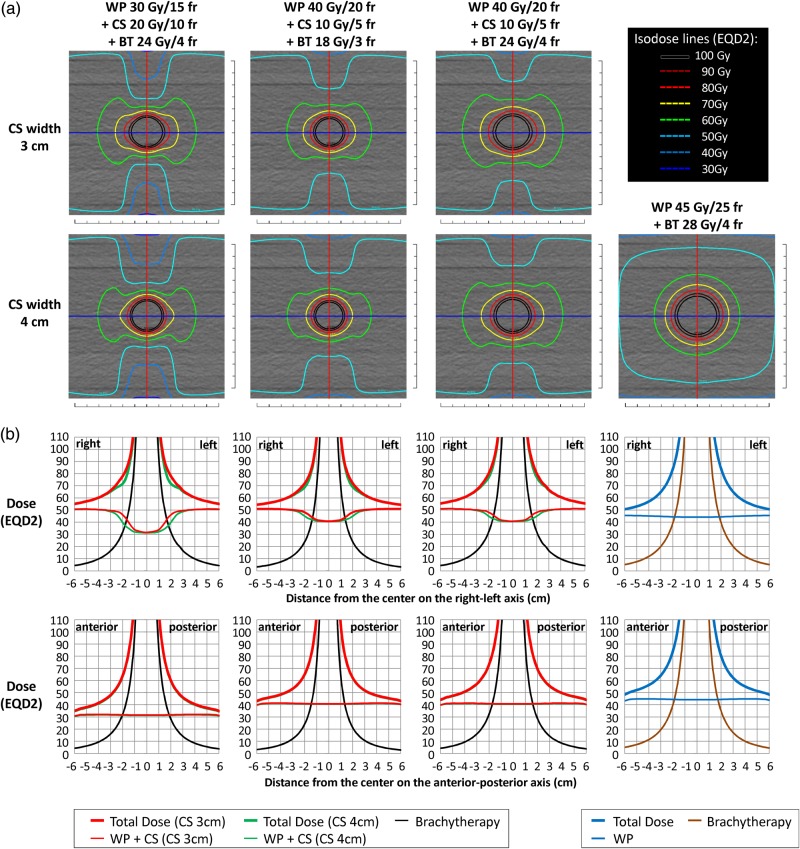
This study aimed to provide accurate dose distribution profiles of radiotherapy for cervical cancer when treated with the central shielding technique by analysing the composite 3D EQD2 dose distribution of external beam radiotherapy (EBRT) plus intracavitary brachytherapy (ICBT). On a phantom, four patterns of the combinations of whole pelvis irradiation (WP) (4 fields), pelvis irradiation with central shielding technique (CS) [anterior-posterior/posterior-anterior (AP-PA fields), shielding width of 3 or 4 cm] and ICBT using Point-A prescription were created: 30 Gy/15 fractions + 20 Gy/10 fractions + 24 Gy/4 fractions [Plan (30 + 20 + 24)], 40 Gy/20 fractions + 10 Gy/5 fractions + 18 Gy/3 fractions [Plan (40 + 10 + 18)], 40 Gy/20 fractions + 10 Gy/5 fractions + 24 Gy/4 fractions [Plan (40 + 10 + 24)] and 45 Gy/25 fractions + 0 Gy + 28 Gy/4 fractions [Plan (45 + 0 + 28)]. The composite EQD2 dose distributions of the complete treatment were analysed. The Point-A dose of Plan (30 + 20 + 24), Plan (40 + 10 + 18), Plan (40 + 10 + 24) and Plan (45 + 0 + 28) were 78.0 Gy (CS 3 cm)/71.8 Gy (CS 4 cm), 72.1 Gy (CS 3 cm)/69.0 Gy (CS 4 cm), 80.1 Gy (CS 3 cm)/77.0 Gy (CS 4 cm) and 84.1 Gy, whereas it has been previously reported to be 62 Gy, 64 Gy, 72 Gy and 84 Gy, respectively. For all the treatment plans with CS, equivalent or wider coverage of 60 Gy (EQD2) was achieved in the right-left direction, while coverage in the anterior-posterior direction decreased in plans with CS. There were no irregularly 'cold' regions around the central target. The use of CS in radiotherapy for cervical cancer resulted in tumor coverage in the lateral direction with doses higher than the previously reported Point-A doses.
本研究旨在通过分析外照射放疗(EBRT)联合腔内近距离放疗(ICBT)的复合三维等效均匀剂量(EQD2)剂量分布,提供宫颈癌采用中央屏蔽技术治疗时准确的放疗剂量分布概况。在体模上,创建了全盆腔照射(WP)(4野)、采用中央屏蔽技术(CS)的盆腔照射[前后/后前(AP-PA野),屏蔽宽度3或4 cm]以及使用A点处方的ICBT的四种组合模式:30 Gy/15次分割 + 20 Gy/10次分割 + 24 Gy/4次分割[方案(30 + 20 + 24)]、40 Gy/20次分割 + 10 Gy/5次分割 + 18 Gy/3次分割[方案(40 + 10 + 18)]、40 Gy/20次分割 + 10 Gy/5次分割 + 24 Gy/4次分割[方案(40 + 10 + 24)]和45 Gy/25次分割 + 0 Gy + 28 Gy/4次分割[方案(45 + 0 + 28)]。分析了完整治疗的复合EQD2剂量分布。方案(30 + 20 + 24)、方案(40 + 10 + 18)、方案(40 + 10 + 24)和方案(45 + 0 + 28)的A点剂量分别为78.0 Gy(CS 3 cm)/71.8 Gy(CS 4 cm)、72.1 Gy(CS 3 cm)/69.0 Gy(CS 4 cm)、80.1 Gy(CS 3 cm)/77.0 Gy(CS 4 cm)和84.1 Gy,而此前报道分别为62 Gy、64 Gy、72 Gy和84 Gy。对于所有采用CS的治疗方案,在左右方向上实现了60 Gy(EQD2)等效或更宽的覆盖范围,而采用CS的方案在前后方向上的覆盖范围减小。中央靶区周围没有不规则的“冷”区。宫颈癌放疗中使用CS导致在侧方方向上肿瘤覆盖范围的剂量高于先前报道的A点剂量。