University of Manchester and Manchester Institute of Nephrology and Transplantation, The Royal Infirmary, Manchester, UK.
Sheffield Kidney Institute, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK.
Clin Kidney J. 2012 Feb;5(Suppl 1):i62-i70. doi: 10.1093/ndtplus/sfr168.
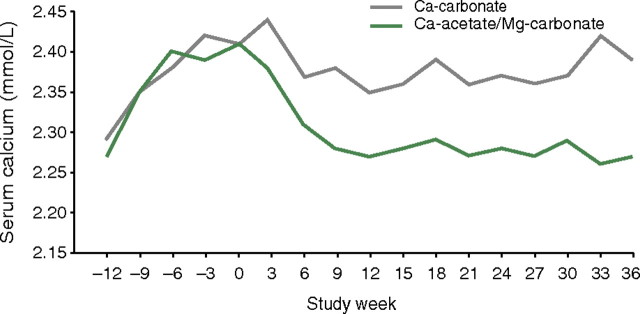
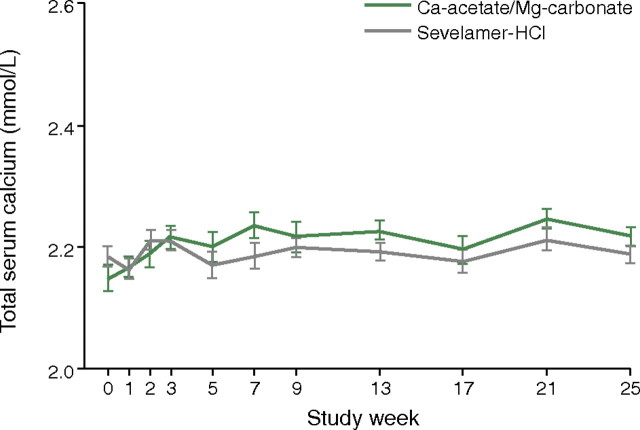
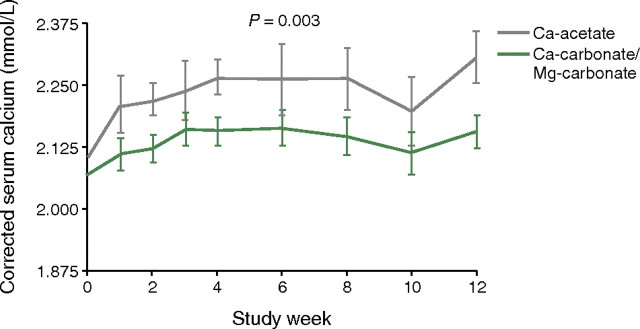
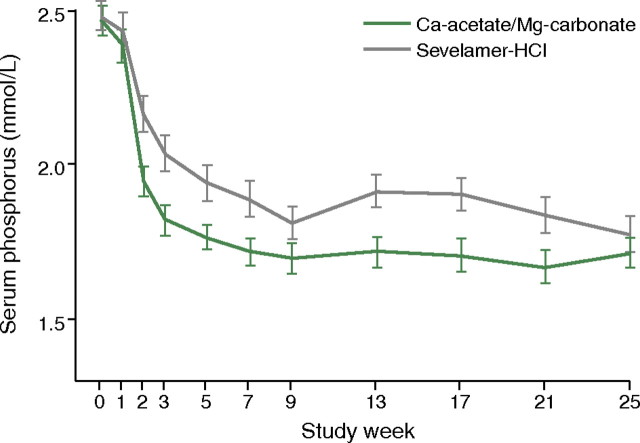
From chronic kidney disease (CKD) Stage 4 onwards, phosphate binders are needed in many patients to prevent the development of hyperphosphataemia, which can result in disturbed bone and mineral metabolism, cardiovascular disease and secondary hyperparathyroidism. In this review, we re-examine the use of magnesium-containing phosphate binders for patients with CKD, particularly as their use circumvents problems such as calcium loading, aluminum toxicity and the high costs associated with other agents of this class. The use of magnesium hydroxide in the 1980s has been superseded by magnesium carbonate, as the hydroxide salt was associated with poor gastrointestinal tolerability, whereas studies with magnesium carbonate show much better gastrointestinal profiles. The use of combined magnesium- and calcium-based phosphate binder regimens allows a reduction in the calcium load, and magnesium and calcium regimen comparisons show that magnesium may be as effective a phosphate binder as calcium. A large well-designed trial has recently shown that a drug combining calcium acetate and magnesium carbonate was non-inferior in terms of lowering serum phosphate to sevelamer-HCl and had an equally good tolerability profile. Because of the high cost of sevelamer and lanthanum carbonate, the use of magnesium carbonate could be advantageous and drug acquisition cost savings would compensate for the cost of introducing routine magnesium monitoring, if this is thought to be necessary and not performed anyway. Moreover, given the potential cost savings, it may be time to re-investigate magnesium-containing phosphate binders for CKD patients with further well-designed clinical research using vascular end points.
从慢性肾脏病(CKD)第 4 期开始,许多患者需要使用磷酸盐结合剂来预防高磷血症的发生,因为高磷血症会导致骨和矿物质代谢紊乱、心血管疾病和继发性甲状旁腺功能亢进。在这篇综述中,我们重新审视了含镁磷酸盐结合剂在 CKD 患者中的应用,特别是因为它们的使用可以避免钙负荷、铝毒性和与该类其他药物相关的高成本等问题。镁氢氧化物在 20 世纪 80 年代的应用已经被碳酸镁所取代,因为氢氧化物盐与较差的胃肠道耐受性有关,而碳酸镁的研究则显示出更好的胃肠道特性。联合使用镁和钙基磷酸盐结合剂方案可以减少钙负荷,并且镁和钙方案的比较表明,镁作为磷酸盐结合剂可能与钙一样有效。最近的一项大型精心设计的试验表明,一种联合醋酸钙和碳酸镁的药物在降低血清磷酸盐方面与司维拉姆盐酸盐相比不劣效,并且具有同样良好的耐受性。由于司维拉姆和碳酸镧的成本较高,因此使用碳酸镁可能具有优势,如果认为有必要且无论如何都不进行常规镁监测,则药物获取成本节省可以弥补引入常规镁监测的成本。此外,考虑到潜在的成本节约,可能是时候重新研究含镁磷酸盐结合剂在进一步使用血管终点进行精心设计的临床研究的 CKD 患者中的应用了。