Tzankov Alexandar, Leu Nora, Muenst Simone, Juskevicius Darius, Klingbiel Dirk, Mamot Christoph, Dirnhofer Stephan
Institute of Pathology, University Hospital Basel, Schoenbeinstrasse 40, CH-4031, Basel, Switzerland.
Swiss Group for Clinical Cancer Research (SAKK), Effingerstrasse 40, CD-3008, Bern, Switzerland.
J Hematol Oncol. 2015 Jun 14;8:70. doi: 10.1186/s13045-015-0168-7.
The prognostic role of tumor-related parameters in diffuse large B cell lymphoma (DLBCL) is a matter of controversy.
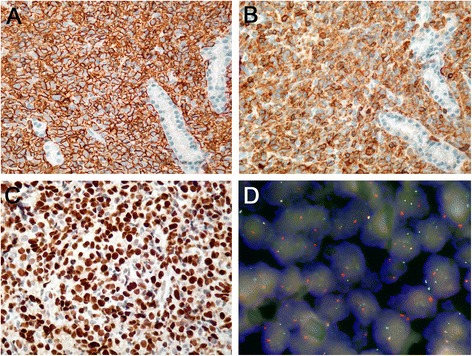
We investigated the prognostic value of phenotypic and genotypic profiles in DLBCL in clinical trial (NCT00544219) patients homogenously treated with six cycles of rituximab, cyclophosphamide, hydroxydaunorubicin, vincristine, prednisone (R-CHOP), followed by two cycles of R (R-CHOP-14). The primary endpoint was event-free survival at 2 years (EFS). Secondary endpoints were progression-free (PFS) and overall survival (OS). Immunohistochemical (bcl2, bcl6, CD5, CD10, CD20, CD95, CD168, cyclin E, FOXP1, GCET, Ki-67, LMO2, MUM1p, pSTAT3) and in situ hybridization analyses (BCL2 break apart probe, C-MYC break apart probe and C-MYC/IGH double-fusion probe, and Epstein-Barr virus probe) were performed and correlated with the endpoints.
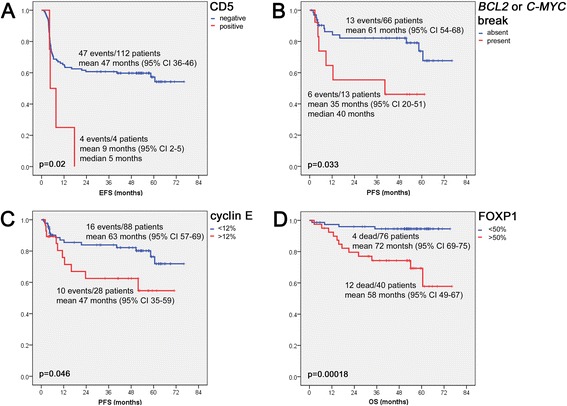
One hundred twenty-three patients (median age 58 years) were evaluable. Immunohistochemical assessment succeeded in all cases. Fluorescence in situ hybridization was successful in 82 instances. According to the Tally algorithm, 81 cases (66%) were classified as non-germinal center (GC) DLBCL, while 42 cases (34%) were GC DLBCL. BCL2 gene breaks were observed in 7/82 cases (9%) and C-MYC breaks in 6/82 cases (8%). "Double-hit" cases with BCL2 and C-MYC rearrangements were not observed. Within the median follow-up of 53 months, there were 51 events, including 16 lethal events and 12 relapses. Factors able to predict worse EFS in univariable models were failure to achieve response according to international criteria, failure to achieve positron emission tomography response (p < 0.005), expression of CD5 (p = 0.02), and higher stage (p = 0.021). Factors predicting inferior PFS were failure to achieve response according to international criteria (p < 0.005), higher stage (p = 0.005), higher International Prognostic Index (IPI; p = 0.006), and presence of either C-MYC or BCL2 gene rearrangements (p = 0.033). Factors predicting inferior OS were failure to achieve response according to international criteria and expression of FOXP1 (p < 0.005), cyclin E, CD5, bcl2, CD95, and pSTAT3 (p = 0.005, 0.007, 0.016, and 0.025, respectively). Multivariable analyses revealed that expression of CD5 (p = 0.044) and FOXP1 (p = 0.004) are independent prognostic factors for EFS and OS, respectively.
Phenotypic studies with carefully selected biomarkers like CD5 and FOXP1 are able to prognosticate DLBCL course at diagnosis, independent of stage and IPI and independent of response to R-CHOP.
肿瘤相关参数在弥漫性大B细胞淋巴瘤(DLBCL)中的预后作用存在争议。
我们在一项临床试验(NCT00544219)中研究了DLBCL患者的表型和基因型谱的预后价值,这些患者均接受了六个周期的利妥昔单抗、环磷酰胺、羟基柔红霉素、长春新碱、泼尼松(R-CHOP)治疗,随后进行两个周期的R(R-CHOP-14)治疗。主要终点是2年无事件生存期(EFS)。次要终点是无进展生存期(PFS)和总生存期(OS)。进行了免疫组织化学(bcl2、bcl6、CD5、CD10、CD20、CD95、CD168、细胞周期蛋白E、FOXP1、GCET、Ki-67、LMO2、MUM1p、pSTAT3)和原位杂交分析(BCL2断裂探针、C-MYC断裂探针和C-MYC/IGH双融合探针,以及爱泼斯坦-巴尔病毒探针),并将其与终点相关联。
123例患者(中位年龄58岁)可进行评估。免疫组织化学评估在所有病例中均成功。荧光原位杂交在82例中成功。根据Tally算法,81例(66%)被分类为非生发中心(GC)DLBCL,而42例(34%)为GC DLBCL。在82例中的7例(9%)观察到BCL2基因断裂,在82例中的6例(8%)观察到C-MYC断裂。未观察到BCL2和C-MYC重排的“双打击”病例。在中位随访53个月期间,有51个事件,包括16个致命事件和12个复发事件。在单变量模型中能够预测较差EFS的因素是未根据国际标准达到缓解、未达到正电子发射断层扫描反应(p<0.005)、CD5表达(p=0.02)和更高分期(p=0.021)。预测较差PFS的因素是未根据国际标准达到缓解(p<0.005)、更高分期(p=0.005)、更高国际预后指数(IPI;p=0.006)以及存在C-MYC或BCL2基因重排(p=0.033)。预测较差OS的因素是未根据国际标准达到缓解以及FOXP1表达(p<0.005)、细胞周期蛋白E、CD5、bcl2、CD95和pSTAT3(分别为p=0.005、0.007、0.016和0.025)。多变量分析显示,CD5表达(p=0.044)和FOXP1表达(p=0.004)分别是EFS和OS的独立预后因素。
使用精心挑选的生物标志物如CD5和FOXP1进行表型研究能够在诊断时预测DLBCL病程,独立于分期和IPI,且独立于对R-CHOP的反应。