Zhang Sai, Bastian Nathaniel D, Griffin Paul M
Department of Industrial Engineering, Penn State University, University Park, PA, 16803, USA.
School of Industrial and Systems Engineering, Georgia Institute of Technology, 755 Ferst Dr, Atlanta, GA, 30332-0205, USA.
BMC Gastroenterol. 2015 Aug 5;15:98. doi: 10.1186/s12876-015-0320-4.
The standard care of treatment of interferon plus ribavirin (plus protease inhibitor for genotype 1) are effective in 50 % to 70 % of patients with CHC. Several new treatments including Harvoni, Olysio + Sovaldi, Viekira Pak, Sofosbuvir-based regimens characterized with potent inhibitors have been approved by the Food and Drug Administration (FDA) providing more options for CHC patients. Trials have shown that the new treatments increased the rate to 80% to 95%, though with a substantial increase in cost. In particular, current market pricing of a 12-week course of sofosbuvir is approximately US$84,000. We determine the cost-effectiveness of new treatments in comparison with the standard care of treatments.
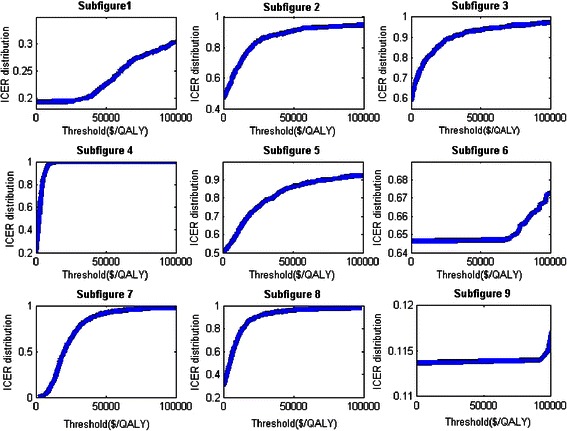
A Markov simulation model of CHC disease progression is used to evaluate the cost-effectiveness of different treatment strategies based on genotype. The model calculates the expected lifetime medical costs and quality adjusted life years (QALYs) of hypothetical cohorts of identical patients receiving certain treatments. For genotype 1, we compare: (1) peginterferon + ribavirin + telaprevir for 12 weeks, followed by 12 or 24 weeks treatment of peginterferon + ribavirin dependent on HCV RNA level at week 12; (2) Harvoni treatment, 12 weeks; (3) Olysio + Sovaldi, 12 weeks for patients without cirrhosis, 24 weeks for patients with cirrhosis; (4) Viekira Pak + ribavirin, 12 weeks for patients without cirrhosis, 24 weeks for patients with cirrhosis; (5) sofosbuvir + peginterferon + ribavirin, 12 weeks for patients with or without cirrhosis. For genotypes 2 and 3, treatment strategies include: (1) peginterferon + ribavirin, 24 weeks for treatment-naïve patients; (2) sofosbuvir + ribavirin, 12 weeks for patients with genotype 2, 24 weeks for genotype 3; (3) peginterferon + ribavirin as initial treatment, 24 weeks for patients with genotype 2/3, follow-up treatment with sofosbuvir + ribavirin for 12/16 weeks are performed on non-responders and relapsers.
Viekira Pak is cost-effective for genotype 1 patients without cirrhosis, whereas Harvoni is cost-effective for genotype 1 patients with cirrhosis. Sofosbuvir-based treatments for genotype 1 in general are not cost-effective due to its substantial high costs. Two-phase treatments with 12-week and 16-week follow-ups are cost-effective for genotype 3 patients and for genotype 2 patients with cirrhosis. The results were shown to be robust over a broad range of parameter values through sensitivity analysis.
For genotype 1, sofosbuvir-based treatments are not cost-effective compared to Viekira Pak and Harvoni, although a 30% reduction in sofosbuvir price would change this result. Sofosbuvir + ribavirin are cost-effective as second-phase treatments following peginterferon + ribavirin initial treatment for genotypes 2 and 3. However, there is limited data on sofosbuvir-involved treatment, and the results obtained in this study must be interpreted within the model assumptions.
干扰素加利巴韦林(基因1型患者加用蛋白酶抑制剂)的标准治疗方案对50%至70%的慢性丙型肝炎(CHC)患者有效。包括哈瓦尼(Harvoni)、欧利希(Olysio)+索华迪(Sovaldi)、维柯帕克(Viekira Pak)、以索非布韦为基础且含有强效抑制剂的治疗方案在内的几种新疗法已获美国食品药品监督管理局(FDA)批准,为CHC患者提供了更多选择。试验表明,新疗法将治愈率提高到了80%至95%,不过成本大幅增加。特别是,目前一个12周疗程的索非布韦市场定价约为84,000美元。我们比较新疗法与标准治疗方案的成本效益。
采用CHC疾病进展的马尔可夫模拟模型,基于基因型评估不同治疗策略的成本效益。该模型计算接受特定治疗的相同患者假设队列的预期终身医疗成本和质量调整生命年(QALY)。对于基因1型,我们比较:(1)聚乙二醇干扰素+利巴韦林+特拉匹韦治疗12周,然后根据第12周时的丙型肝炎病毒(HCV)RNA水平,给予聚乙二醇干扰素+利巴韦林治疗12周或24周;(2)哈瓦尼治疗,12周;(3)欧利希+索华迪,无肝硬化患者治疗12周,有肝硬化患者治疗24周;(4)维柯帕克+利巴韦林,无肝硬化患者治疗12周,有肝硬化患者治疗24周;(5)索非布韦+聚乙二醇干扰素+利巴韦林,有或无肝硬化患者均治疗12周。对于基因2型和3型,治疗策略包括:(1)聚乙二醇干扰素+利巴韦林,初治患者治疗24周;(2)索非布韦+利巴韦林,基因2型患者治疗12周,基因3型患者治疗24周;(3)以聚乙二醇干扰素+利巴韦林作为初始治疗,基因2/3型患者治疗24周,对无反应者和复发者采用索非布韦+利巴韦林进行12/16周的后续治疗。
维柯帕克对无肝硬化的基因1型患者具有成本效益,而哈瓦尼对有肝硬化的基因1型患者具有成本效益。基于索非布韦的基因1型治疗方案总体上不具有成本效益,因为其成本过高。对于基因3型患者以及有肝硬化的基因2型患者,采用12周和16周随访的两阶段治疗具有成本效益。通过敏感性分析表明,在广泛的参数值范围内结果是稳健的。
对于基因1型,与维柯帕克和哈瓦尼相比,基于索非布韦的治疗方案不具有成本效益,不过索非布韦价格降低30%会改变这一结果。索非布韦+利巴韦林作为基因2型和3型患者聚乙二醇干扰素+利巴韦林初始治疗后的第二阶段治疗具有成本效益。然而,关于索非布韦相关治疗的数据有限,本研究所得结果必须在模型假设范围内进行解读。