Geisler Tobias, Booth Jean, Tavlaki Elli, Karathanos Athanasios, Müller Karin, Droppa Michal, Gawaz Meinrad, Yanez-Lopez Monica, Davidson Simon J, Stables Rod H, Banya Winston, Zaman Azfar, Flather Marcus, Dalby Miles
Klinikum der Eberhard-Karls-Universität Tübingen, Abteilung für Kardiologie und Kreislauferkrankungen, Tübingen, Germany.
Clinical Trials & Evaluation Unit, Royal Brompton Hospital, London, United Kingdom.
PLoS One. 2015 Aug 28;10(8):e0135037. doi: 10.1371/journal.pone.0135037. eCollection 2015.
Prasugrel is more effective than clopidogrel in reducing platelet aggregation in acute coronary syndromes. Data available on prasugrel reloading in clopidogrel treated patients with high residual platelet reactivity (HRPR) i.e. poor responders, is limited.
To determine the effects of prasugrel loading on platelet function in patients on clopidogrel and high platelet reactivity undergoing percutaneous coronary intervention for acute coronary syndrome (ACS).
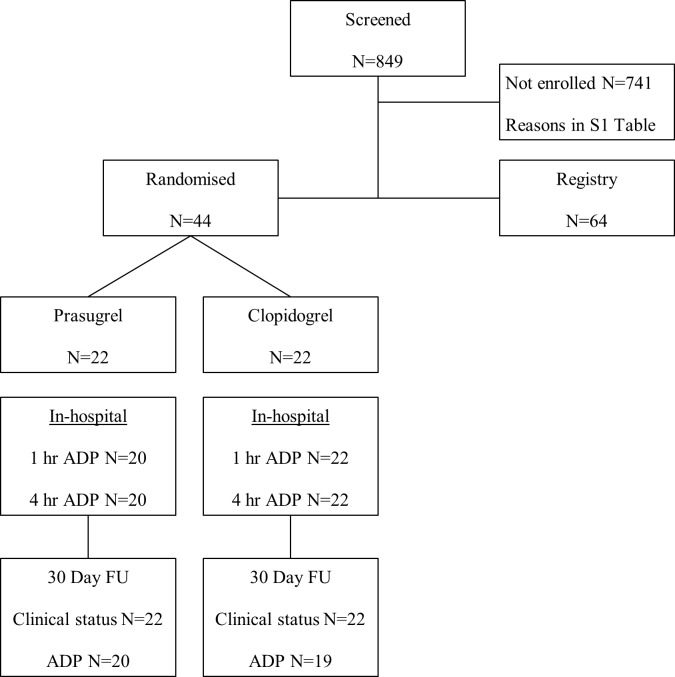
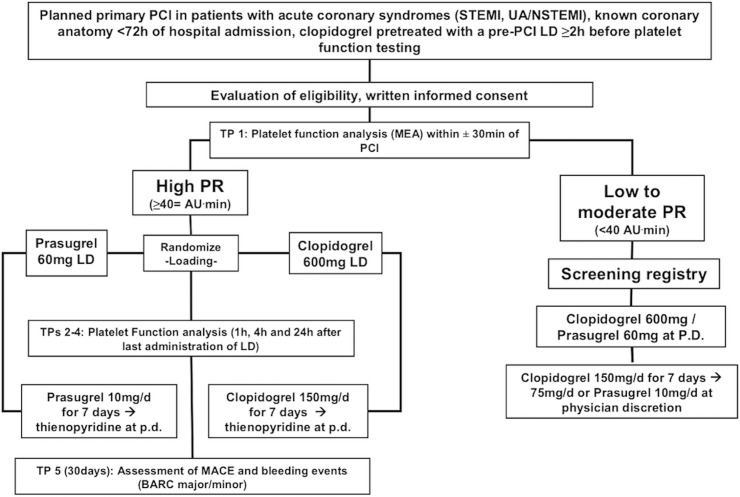
Patients with ACS on clopidogrel who were scheduled for PCI found to have a platelet reactivity ≥40 AUC with the Multiplate Analyzer, i.e. "poor responders" were randomised to prasugrel (60 mg loading and 10 mg maintenance dose) or clopidogrel (600 mg reloading and 150 mg maintenance dose). The primary outcome measure was proportion of patients with platelet reactivity <40 AUC 4 hours after loading with study medication, and also at one hour (secondary outcome). 44 patients were enrolled and the study was terminated early as clopidogrel use decreased sharply due to introduction of newer P2Y12 inhibitors.
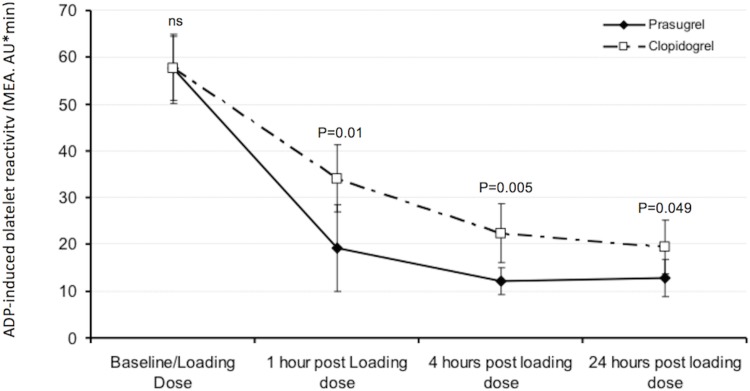
At 4 hours after study medication 100% of patients treated with prasugrel compared to 91% of those treated with clopidogrel had platelet reactivity <40 AUC (p = 0.49), while at 1 hour the proportions were 95% and 64% respectively (p = 0.02). Mean platelet reactivity at 4 and 1 hours after study medication in prasugrel and clopidogrel groups respectively were 12 versus 22 (p = 0.005) and 19 versus 34 (p = 0.01) respectively.
Routine platelet function testing identifies patients with high residual platelet reactivity ("poor responders") on clopidogrel. A strategy of prasugrel rather than clopidogrel reloading results in earlier and more sustained suppression of platelet reactivity. Future trials need to identify if this translates into clinical benefit.
ClinicalTrials.gov NCT01339026.
在急性冠脉综合征中,普拉格雷在降低血小板聚集方面比氯吡格雷更有效。关于在氯吡格雷治疗的高残余血小板反应性(HRPR)患者(即反应不佳者)中重新加载普拉格雷的数据有限。
确定在接受氯吡格雷治疗且血小板反应性高的急性冠脉综合征(ACS)患者中,接受经皮冠状动脉介入治疗时加载普拉格雷对血小板功能的影响。
计划接受PCI的氯吡格雷治疗的ACS患者,通过多电极血小板聚集分析仪检测发现血小板反应性≥40 AUC,即“反应不佳者",被随机分为普拉格雷组(负荷剂量60 mg,维持剂量10 mg)或氯吡格雷组(重新加载剂量600 mg,维持剂量150 mg)。主要结局指标是在加载研究药物后4小时血小板反应性<40 AUC的患者比例,1小时时的情况作为次要结局。共纳入44例患者,由于新型P2Y12抑制剂的引入,氯吡格雷的使用急剧减少,该研究提前终止。
在研究药物治疗后4小时,接受普拉格雷治疗的患者中有100%的血小板反应性<40 AUC,而接受氯吡格雷治疗的患者中这一比例为91%(p = 0.49);在1小时时,相应比例分别为95%和64%(p = 0.02)。普拉格雷组和氯吡格雷组在研究药物治疗后4小时和1小时的平均血小板反应性分别为12对22(p = 0.005)和19对34(p = 0.01)。
常规血小板功能检测可识别出氯吡格雷治疗下具有高残余血小板反应性(“反应不佳者”)的患者。采用普拉格雷而非氯吡格雷重新加载的策略可更早、更持续地抑制血小板反应性。未来的试验需要确定这是否能转化为临床益处。
ClinicalTrials.gov NCT01339026。