Barennes Hubert, Frichittavong Amphonexay, Gripenberg Marissa, Koffi Paulin
Institut de la Francophonie pour la Médecine Tropicale, Vientiane, Lao PDR; Epidemiology Unit, Pasteur Institute, Phnom Penh, Cambodia; Agence Nationale de Recherche sur le VIH et les Hépatites, Phnom Penh, Cambodia; ISPED, Centre INSERM U897-Epidemiologie-Biostatistique, Univ. Bordeaux, Bordeaux, France.
Institut de la Francophonie pour la Médecine Tropicale, Vientiane, Lao PDR.
PLoS One. 2015 Sep 1;10(9):e0136664. doi: 10.1371/journal.pone.0136664. eCollection 2015.
The scaling up of antiviral treatment (ART) coverage in the past decade has increased access to care for numerous people living with HIV/AIDS (PLWHA) in low-resource settings. Out-of-pocket payments (OOPs) represent a barrier for healthcare access, adherence and ART effectiveness, and can be economically catastrophic for PLWHA and their family. We evaluated OOPs of PLWHA attending outpatient and inpatient care units and estimated the financial burden for their households in the Lao People's Democratic Republic. We assumed that such OOPs may result in catastrophic health expenses in this context with fragile economical balance and low health insurance coverage.
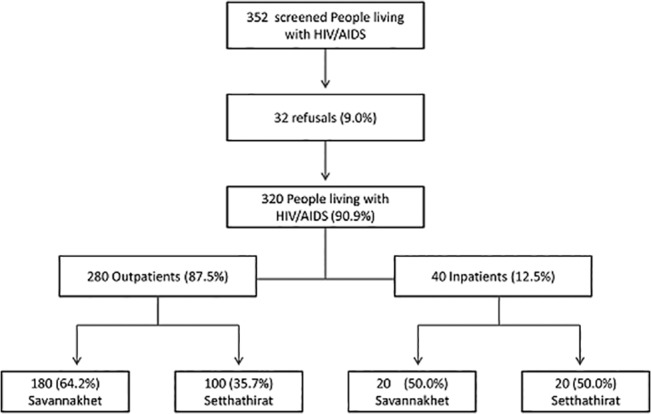
We conducted a cross-sectional survey of a randomized sample of routine outpatients and a prospective survey of consecutive new inpatients at two referral hospitals (Setthathirat in the capital city, Savannaket in the province). After obtaining informed consent, PLWHA were interviewed using a standardized 82-item questionnaire including information on socio-economic characteristics, disease history and coping strategies. All OOPs occurring during a routine visit or a hospital stay were recorded. Household capacity-to-pay (overall income minus essential expenses), direct and indirect OOPs, OOPs per outpatient visit and per inpatient stay as well as catastrophic spending (greater than or equal to 40% of the capacity-to-pay) were calculated. A multivariate analysis of factors associated with catastrophic spending was conducted.
A total of 320 PLWHA [280 inpatients and 40 outpatients; 132 (41.2%) defined as poor, and 269 (84.1%) on ART] were enrolled. Monthly median household income, essential expenses and capacity-to-pay were US$147.0 (IQR: 86-242), $126 (IQR: 82-192) and $14 (IQR: 19-80), respectively. At the provincial hospital OOPs were higher during routine visits, but three fold lower during hospitalization than in the central hospital ($21.0 versus $18.5 and $110.8 versus $329.8 respectively (p<0.01). The most notable OOPs were related to transportation and to loss of income. A total of 150 patients (46.8%; 95%CI: 41.3-52.5) were affected by catastrophic health expenses; 36 outpatients (90.0%; 95%CI: 76.3-97.2) and 114 inpatients (40.7%; 95%CI: 34.9-46.7). A total of 141 (44.0%) patients had contracted loans, and 127 (39.6%) had to sell some of their assets. In the multivariate analysis, being of Lao Loum ethnic group (Coef.-1.4; p = 0.04); being poor (Coef. -1.0; p = 0.01) and living more than 100 km away from the hospital (Coef.-1.0; p = 0.002) were positively associated with catastrophic spending. Conversely being in the highest wealth quartile (Coef. 1.6; p<0.001), living alone (Coef. 1.1; p = 0.04), attending the provincial hospital (Coef. 1.0; p = 0.002), and being on ART (Coef.1.2; p = 0.003), were negatively associated with catastrophic spending.
PLWHA's households face catastrophic OOPs that are not directly attributable to the cost of ART or to follow-up tests, particularly during a hospitalization period. Transportation, distance to healthcare and time spent at the health facility are the major contributors for OOPs and for indirect opportunity costs. Being on ART and attending the provincial hospital were associated with a lower risk of catastrophic spending. Decentralization of care, access to ART and alleviation of OOPs are crucial factors to successfully decrease the household burden of HIV-AIDS expenses.
在过去十年中,扩大抗病毒治疗(ART)覆盖范围使资源匮乏地区众多艾滋病毒/艾滋病感染者(PLWHA)获得了医疗服务。自付费用(OOPs)成为获得医疗服务、坚持治疗和ART疗效的障碍,对PLWHA及其家庭可能造成经济灾难。我们评估了在老挝人民民主共和国就诊于门诊和住院治疗科室的PLWHA的自付费用,并估算了其家庭的经济负担。我们认为,在该国经济平衡脆弱且医疗保险覆盖率低的情况下,此类自付费用可能导致灾难性医疗支出。
我们对两家转诊医院(首都的Setthathirat医院和该省的沙湾拿吉医院)的常规门诊患者随机样本进行了横断面调查,并对连续入院的新患者进行了前瞻性调查。在获得知情同意后,使用一份包含82个项目的标准化问卷对PLWHA进行访谈,问卷内容包括社会经济特征、疾病史和应对策略等信息。记录在常规就诊或住院期间发生的所有自付费用。计算家庭支付能力(总收入减去基本支出)、直接和间接自付费用、每次门诊就诊和每次住院的自付费用以及灾难性支出(大于或等于支付能力的40%)。对与灾难性支出相关的因素进行多变量分析。
共纳入320名PLWHA[280名住院患者和40名门诊患者;132名(41.2%)被界定为贫困,269名(84.1%)接受ART治疗]。家庭月收入中位数、基本支出和支付能力分别为147.0美元(四分位间距:86 - 242美元)、126美元(四分位间距:82 - 192美元)和14美元(四分位间距:19 - 80美元)。在省级医院,常规就诊时的自付费用较高,但住院期间的自付费用比中心医院低三倍(分别为21.0美元对18.5美元以及110.8美元对329.8美元,p<0.01)。最显著的自付费用与交通和收入损失有关。共有150名患者(46.8%;95%置信区间:41.3 - 52.5)受到灾难性医疗支出影响;36名门诊患者(90.0%;95%置信区间:76.3 - 97.2)和114名住院患者(40.7%;95%置信区间:34.9 - 46.7)。共有141名(44.0%)患者借贷,127名(39.6%)患者不得不出售部分资产。在多变量分析中,属于老龙族(系数 -1.4;p = 0.04)、贫困(系数 -1.0;p = 0.01)以及居住在距离医院100公里以上的地方(系数 -1.0;p = 0.002)与灾难性支出呈正相关。相反,处于最高财富四分位数(系数1.6;p<0.001)、独自生活(系数1.1;p = 0.04)、就诊于省级医院(系数1.0;p = 0.002)以及接受ART治疗(系数1.2;p = 0.003)与灾难性支出呈负相关。
PLWHA家庭面临灾难性自付费用,这些费用并非直接归因于ART成本或后续检查,特别是在住院期间。交通、到医疗机构的距离以及在医疗机构花费的时间是自付费用和间接机会成本的主要促成因素。接受ART治疗和就诊于省级医院与较低的灾难性支出风险相关。医疗服务的分散化、获得ART治疗以及减轻自付费用是成功减轻艾滋病毒/艾滋病家庭负担的关键因素。