Lantigua Hector, Ortega-Gutierrez Santiago, Schmidt J Michael, Lee Kiwon, Badjatia Neeraj, Agarwal Sachin, Claassen Jan, Connolly E Sander, Mayer Stephan A
Department of Neurology, Columbia University College of Physicians and Surgeons, 177 Fort Washington Ave, New York, NY, 10032, USA.
Department of Neurology, University of Iowa, 200 Hawkins Drive, Iowa City, IA, 52242, USA.
Crit Care. 2015 Aug 31;19(1):309. doi: 10.1186/s13054-015-1036-0.
Subarachnoid hemorrhage (SAH) is a devastating form of stroke. Causes and mechanisms of in-hospital death after SAH in the modern era of neurocritical care remain incompletely understood.
We studied 1200 consecutive SAH patients prospectively enrolled in the Columbia University SAH Outcomes Project between July 1996 and January 2009. Analysis was performed to identify predictors of in-hospital mortality.
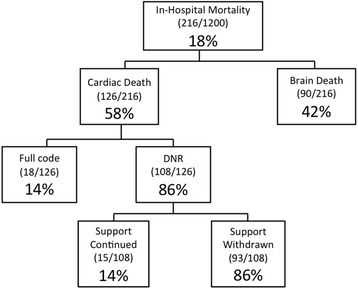
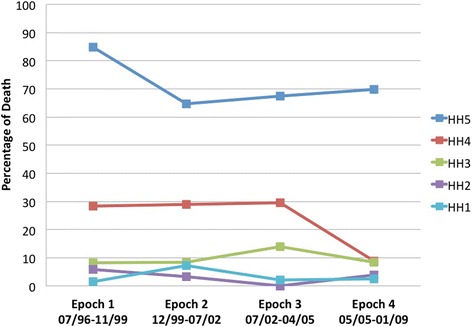
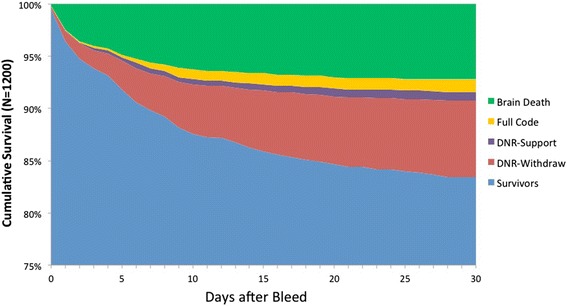
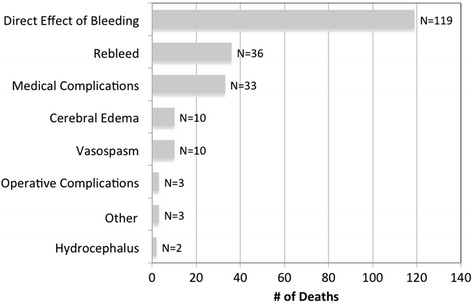
In-hospital mortality was 18% (216/1200): 3% for Hunt-Hess grade 1 or 2, 9% for grade 3, 24% for grade 4, and 71% for grade 5. The most common adjudicated primary causes of death or neurological devastation leading to withdrawal of support were direct effects of the primary hemorrhage (55%), aneurysm rebleeding (17%), and medical complications (15%). Among those who died, brain death was declared in 42%, 50% were do-not-resuscitate at the time of cardiac death (86% of whom had life support actively withdrawn), and 8% died despite full support. Admission predictors of mortality were age, loss of consciousness at ictus, admission Glasgow Coma Scale score, large aneurysm size, Acute Physiology and Chronic Health Evaluation II (APACHE II) physiologic subscore, and Modified Fisher Scale score. Hospital complications that further increased the risk of dying in multivariable analysis included rebleeding, global cerebral edema, hypernatremia, clinical signs of brain stem herniation, hypotension of less than 90 mm Hg treated with pressors, pulmonary edema, myocardial ischemia, and hepatic failure. Delayed cerebral ischemia, defined as deterioration or infarction from vasospasm, did not predict mortality.
Strategies directed toward minimizing early brain injury and aneurysm rebleeding, along with prevention and treatment of medical complication, hold the best promise for further reducing mortality after SAH.
蛛网膜下腔出血(SAH)是一种严重的中风形式。在现代神经重症监护时代,SAH后院内死亡的原因和机制仍未完全明确。
我们前瞻性研究了1996年7月至2009年1月期间连续纳入哥伦比亚大学SAH结局项目的1200例SAH患者。进行分析以确定院内死亡率的预测因素。
院内死亡率为18%(216/1200):Hunt-Hess 1级或2级为3%,3级为9%,4级为24%,5级为71%。导致死亡或因神经功能严重受损而停止支持治疗的最常见经判定的主要原因是原发性出血的直接影响(55%)、动脉瘤再出血(17%)和医疗并发症(15%)。在死亡患者中,42%被宣布脑死亡,50%在心脏死亡时为不进行心肺复苏(其中86%的患者主动撤除生命支持),8%在全力支持治疗下仍死亡。死亡率的入院预测因素包括年龄、发病时意识丧失、入院格拉斯哥昏迷量表评分、动脉瘤较大、急性生理与慢性健康状况评估II(APACHE II)生理子评分和改良Fisher量表评分。在多变量分析中进一步增加死亡风险的医院并发症包括再出血、全脑水肿、高钠血症、脑干疝临床体征、用升压药治疗的收缩压低于90 mmHg的低血压、肺水肿、心肌缺血和肝功能衰竭。定义为因血管痉挛导致病情恶化或梗死的迟发性脑缺血并不能预测死亡率。
旨在将早期脑损伤和动脉瘤再出血降至最低的策略,以及医疗并发症的预防和治疗,对于进一步降低SAH后的死亡率最具前景。