Neogi Tuhina, Jansen Tim L Th A, Dalbeth Nicola, Fransen Jaap, Schumacher H Ralph, Berendsen Dianne, Brown Melanie, Choi Hyon, Edwards N Lawrence, Janssens Hein J E M, Lioté Frédéric, Naden Raymond P, Nuki George, Ogdie Alexis, Perez-Ruiz Fernando, Saag Kenneth, Singh Jasvinder A, Sundy John S, Tausche Anne-Kathrin, Vaquez-Mellado Janitzia, Yarows Steven A, Taylor William J
Boston University School of Medicine, Boston, Massachusetts, USA.
Viecuri Medical Center, Venlo, The Netherlands Radboud University Medical Center, Nijmegen, The Netherlands.
Ann Rheum Dis. 2015 Oct;74(10):1789-98. doi: 10.1136/annrheumdis-2015-208237.
Existing criteria for the classification of gout have suboptimal sensitivity and/or specificity, and were developed at a time when advanced imaging was not available. The current effort was undertaken to develop new classification criteria for gout.
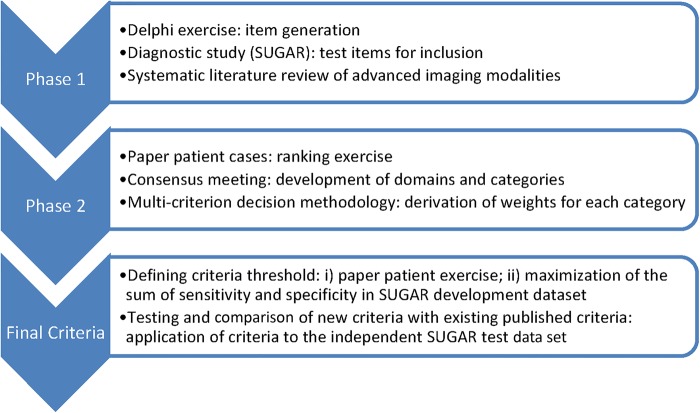
An international group of investigators, supported by the American College of Rheumatology and the European League Against Rheumatism, conducted a systematic review of the literature on advanced imaging of gout, a diagnostic study in which the presence of monosodium urate monohydrate (MSU) crystals in synovial fluid or tophus was the gold standard, a ranking exercise of paper patient cases, and a multi-criterion decision analysis exercise. These data formed the basis for developing the classification criteria, which were tested in an independent data set.
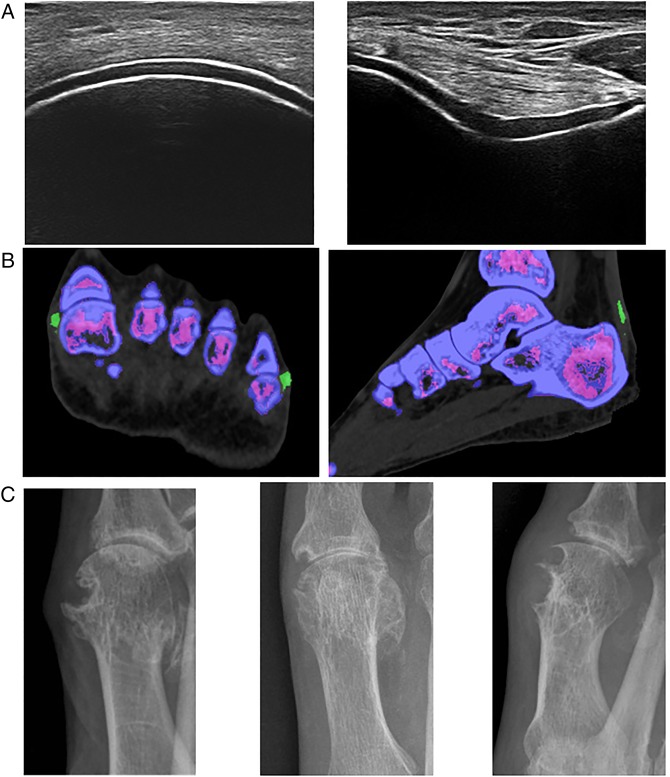
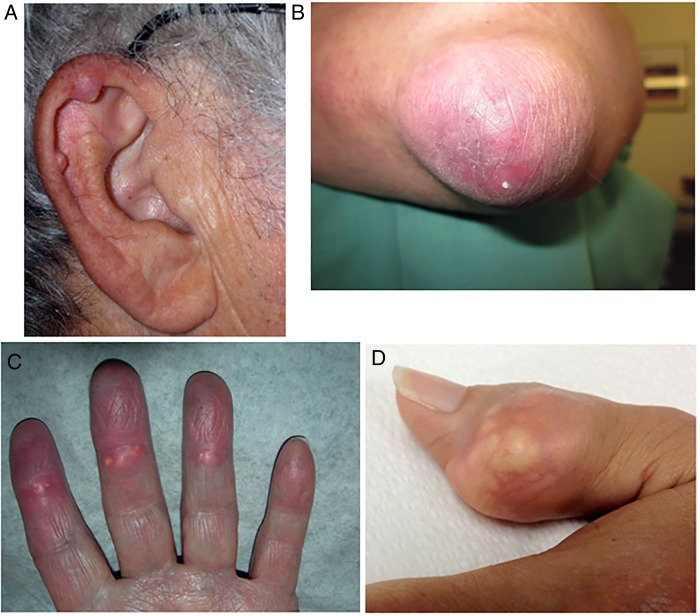
The entry criterion for the new classification criteria requires the occurrence of at least one episode of peripheral joint or bursal swelling, pain, or tenderness. The presence of MSU crystals in a symptomatic joint/bursa (ie, synovial fluid) or in a tophus is a sufficient criterion for classification of the subject as having gout, and does not require further scoring. The domains of the new classification criteria include clinical (pattern of joint/bursa involvement, characteristics and time course of symptomatic episodes), laboratory (serum urate, MSU-negative synovial fluid aspirate), and imaging (double-contour sign on ultrasound or urate on dual-energy CT, radiographic gout-related erosion). The sensitivity and specificity of the criteria are high (92% and 89%, respectively).
The new classification criteria, developed using a data-driven and decision-analytic approach, have excellent performance characteristics and incorporate current state-of-the-art evidence regarding gout.
现有的痛风分类标准敏感性和/或特异性欠佳,且是在先进成像技术尚未出现时制定的。当前开展此项工作旨在制定新的痛风分类标准。
一个由国际研究人员组成的团队,在美国风湿病学会和欧洲抗风湿病联盟的支持下,对痛风的先进成像相关文献进行了系统综述,开展了一项以滑液或痛风石中存在单水尿酸钠(MSU)晶体为金标准的诊断研究、一次纸质患者病例排序活动以及一次多标准决策分析活动。这些数据构成了制定分类标准的基础,并在一个独立数据集中进行了测试。
新分类标准的纳入标准要求至少出现一次外周关节或滑囊肿胀、疼痛或压痛发作。有症状的关节/滑囊(即滑液)或痛风石中存在MSU晶体是将受试者分类为患有痛风的充分标准,无需进一步评分。新分类标准的领域包括临床(关节/滑囊受累模式、症状发作的特征和时间进程)、实验室(血清尿酸、MSU阴性的滑液抽吸物)和影像学(超声上的双轮廓征或双能CT上的尿酸盐、与痛风相关的放射学侵蚀)。该标准的敏感性和特异性很高(分别为92%和89%)。
采用数据驱动和决策分析方法制定的新分类标准具有出色的性能特征,并纳入了有关痛风的当前最新证据。