Jin Byung-Soo, Kang Seok-Hyun, Kim Duk-Yoon, Oh Hoon-Gyu, Kim Chun-Il, Moon Gi-Hak, Kwon Tae-Gyun, Park Jae-Shin
Department of Urology, Catholic University of Daegu School of Medicine, Daegu, Korea.
Department of Pathology, Catholic University of Daegu School of Medicine, Daegu, Korea.
Korean J Urol. 2015 Sep;56(9):624-9. doi: 10.4111/kju.2015.56.9.624. Epub 2015 Sep 2.
To evaluate prospectively the role of prostate-specific antigen (PSA) density in predicting Gleason score upgrading in prostate cancer patients eligible for active surveillance (T1/T2, biopsy Gleason score≤6, PSA≤10 ng/mL, and ≤2 positive biopsy cores).
Between January 2010 and November 2013, among patients who underwent greater than 10-core transrectal ultrasound-guided biopsy, 60 patients eligible for active surveillance underwent radical prostatectomy. By use of the modified Gleason criteria, the tumor grade of the surgical specimens was examined and compared with the biopsy results.
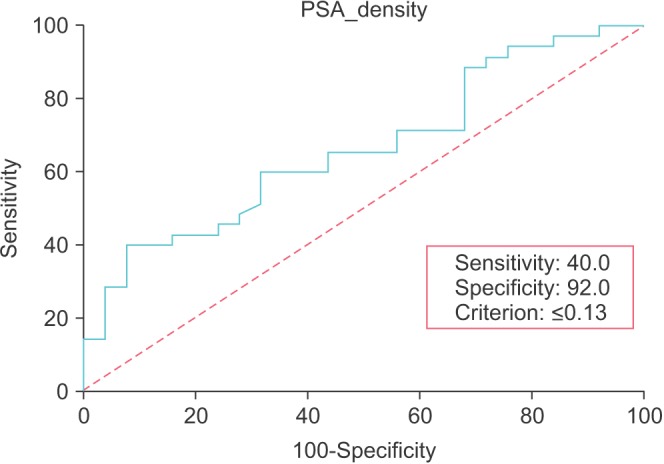
Tumor upgrading occurred in 24 patients (40.0%). Extracapsular disease and positive surgical margins were found in 6 patients (10.0%) and 8 patients (17.30%), respectively. A statistically significant correlation between PSA density and postoperative upgrading was found (p=0.030); this was in contrast with the other studied parameters, which failed to reach significance, including PSA, prostate volume, number of biopsy cores, and number of positive cores. Tumor upgrading was also highly associated with extracapsular cancer extension (p=0.000). The estimated optimal cutoff value of PSA density was 0.13 ng/mL(2), obtained by receiver operating characteristic analysis (area under the curve=0.66; p=0.020; 95% confidence interval, 0.53-0.78).
PSA density is a strong predictor of Gleason score upgrading after radical prostatectomy in patients eligible for active surveillance. Because tumor upgrading increases the potential for postoperative pathological adverse findings and prognosis, PSA density should be considered when treating and consulting patients eligible for active surveillance.
前瞻性评估前列腺特异性抗原(PSA)密度在预测适合主动监测的前列腺癌患者(T1/T2期,活检Gleason评分≤6分,PSA≤10 ng/mL,且活检阳性核心数≤2个)Gleason评分升级中的作用。
2010年1月至2013年11月期间,在接受超过10针经直肠超声引导下活检的患者中,60例适合主动监测的患者接受了根治性前列腺切除术。采用改良Gleason标准,检查手术标本的肿瘤分级并与活检结果进行比较。
24例患者(40.0%)出现肿瘤分级升级。分别有6例患者(10.0%)和8例患者(17.30%)发现包膜外侵犯和手术切缘阳性。发现PSA密度与术后分级升级之间存在统计学显著相关性(p=0.030);这与其他研究参数形成对比,其他参数未达到显著水平,包括PSA、前列腺体积、活检针数和阳性针数。肿瘤分级升级也与包膜外癌扩展高度相关(p=0.000)。通过受试者操作特征分析获得的PSA密度估计最佳截断值为0.13 ng/mL²(曲线下面积=0.66;p=0.020;95%置信区间,0.53 - 0.78)。
PSA密度是适合主动监测的患者根治性前列腺切除术后Gleason评分升级的有力预测指标。由于肿瘤分级升级会增加术后病理不良发现和预后的可能性,在治疗和咨询适合主动监测的患者时应考虑PSA密度。