Chinnakotla Srinath, Beilman Gregory J, Dunn Ty B, Bellin Melena D, Freeman Martin L, Radosevich David M, Arain Mustafa, Amateau Stuart K, Mallery J Shawn, Schwarzenberg Sarah J, Clavel Alfred, Wilhelm Joshua, Robertson R Paul, Berry Louise, Cook Marie, Hering Bernhard J, Sutherland David E R, Pruett Timothy L
*Department of Surgery, University of Minnesota Medical School, Minneapolis, MN †Department of Pediatrics, University of Minnesota Medical School, Minneapolis, MN ‡Schulze Diabetes Institute, University of Minnesota Medical School, Minneapolis, MN §Department of Medicine, University of Minnesota Medical School, Minneapolis, MN ¶Pain Management, University of Minnesota Medical School, Minneapolis, MN.
Ann Surg. 2015 Oct;262(4):610-22. doi: 10.1097/SLA.0000000000001453.
Our objective was to analyze factors predicting outcomes after a total pancreatectomy and islet autotransplantation (TP-IAT).
Chronic pancreatitis (CP) is increasingly treated by a TP-IAT. Postoperative outcomes are generally favorable, but a minority of patients fare poorly.
In our single-centered study, we analyzed the records of 581 patients with CP who underwent a TP-IAT. Endpoints included persistent postoperative "pancreatic pain" similar to preoperative levels, narcotic use for any reason, and islet graft failure at 1 year.
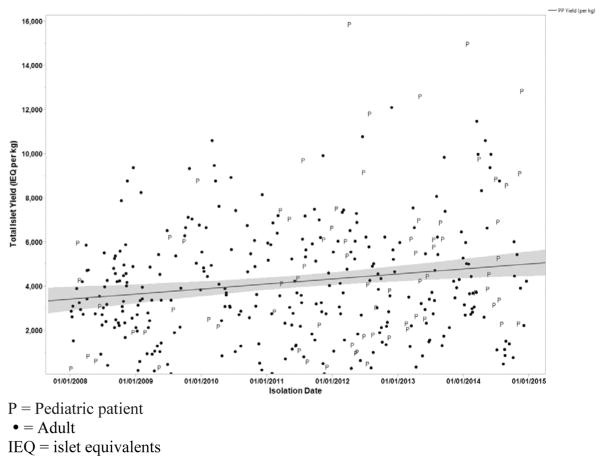
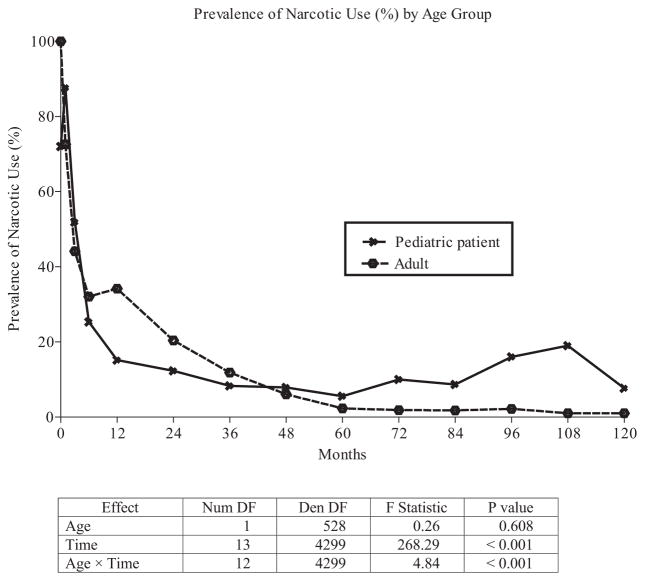
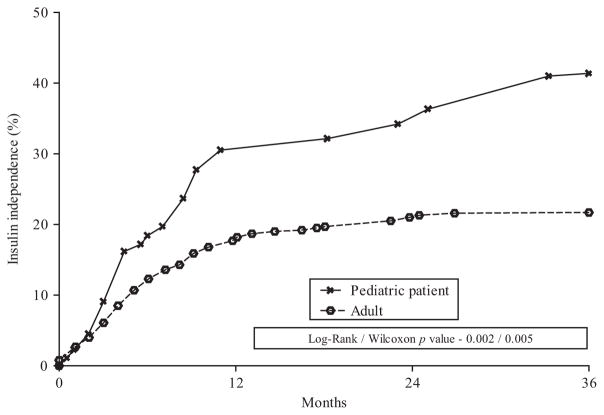
In our patients, the duration (mean ± SD) of CP before their TP-IAT was 7.1 ± 0.3 years and narcotic usage of 3.3 ± 0.2 years. Pediatric patients had better postoperative outcomes. Among adult patients, the odds of narcotic use at 1 year were increased by previous endoscopic retrograde cholangiopancreatography (ERCP) and stent placement, and a high number of previous stents (>3). Independent risk factors for pancreatic pain at 1 year were pancreas divisum, previous body mass index >30, and a high number of previous stents (>3). The strongest independent risk factor for islet graft failure was a low islet yield-in islet equivalents (IEQ)-per kilogram of body weight. We noted a strong dose-response relationship between the lowest-yield category (<2000 IEQ) and the highest (≥5000 IEQ or more). Islet graft failure was 25-fold more likely in the lowest-yield category.
This article represents the largest study of factors predicting outcomes after a TP-IAT. Preoperatively, the patient subgroups we identified warrant further attention.
我们的目的是分析全胰切除术及胰岛自体移植(TP-IAT)后预测预后的因素。
慢性胰腺炎(CP)越来越多地通过TP-IAT进行治疗。术后结果总体良好,但少数患者预后较差。
在我们的单中心研究中,我们分析了581例行TP-IAT的CP患者的记录。终点包括术后持续存在与术前水平相似的“胰腺疼痛”、因任何原因使用麻醉剂以及1年时胰岛移植失败。
在我们的患者中,TP-IAT前CP的病程(均值±标准差)为7.1±0.3年,麻醉剂使用时间为3.3±0.2年。儿科患者术后结果更好。在成年患者中,既往进行内镜逆行胰胆管造影(ERCP)和支架置入以及既往支架数量较多(>3个)会增加1年时使用麻醉剂的几率。1年时胰腺疼痛的独立危险因素包括胰腺分裂、既往体重指数>30以及既往支架数量较多(>3个)。胰岛移植失败的最强独立危险因素是每千克体重的胰岛产量低——以胰岛当量(IEQ)计。我们注意到最低产量类别(<2000 IEQ)与最高产量类别(≥5000 IEQ或更高)之间存在强烈的剂量反应关系。最低产量类别中胰岛移植失败的可能性高出25倍。
本文是关于TP-IAT后预测预后因素的最大规模研究。术前,我们确定的患者亚组值得进一步关注。