El-Cheikh Jean, Crocchiolo Roberto, Vai Andrea, Furst Sabine, Bramanti Stefania, Sarina Barbara, Granata Angela, Faucher Catherine, Mohty Bilal, Harbi Samia, Bouabdallah Reda, Vey Norbert, Santoro Armando, Chabannon Christian, Castagna Luca, Blaise Didier
Unité de Transplantation et de Thérapie Cellulaire (U2T), Institut Paoli-Calmettes, Marseille, France ; Departement d'Onco-Hématologie, Institut Paoli-Calmettes, Marseille, France.
Humanitas cancer Centre, Milan, Rozzano, Italy.
Mediterr J Hematol Infect Dis. 2015 Aug 20;7(1):e2015048. doi: 10.4084/MJHID.2015.048. eCollection 2015.
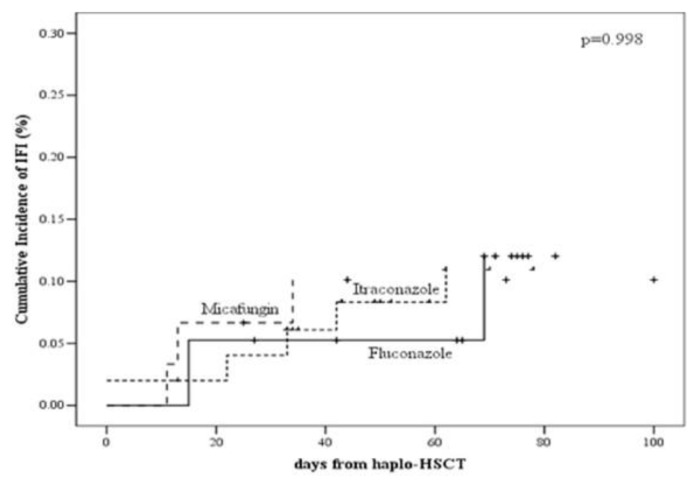
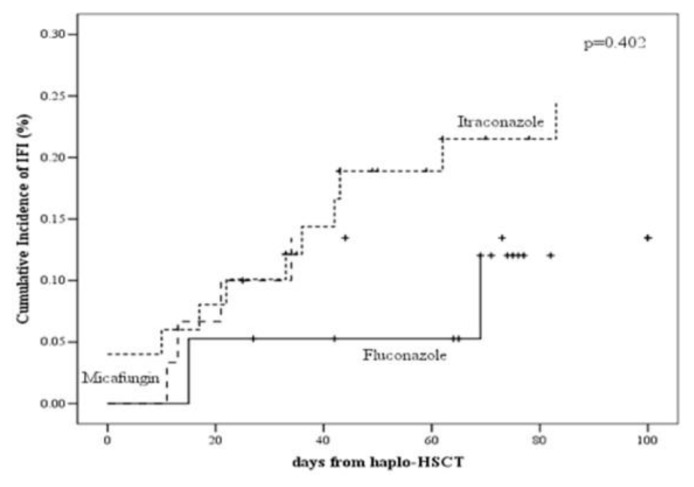
Over the past decade, invasive fungal infections (IFIs) have remained an important problem in patients undergoing allogeneic haematopoietic stem cell transplantation (Allo-HSCT). The optimal approach for prophylactic antifungal therapy has yet to bedetermined. We conducted a retrospective analysis, comparing the safety and efficacy of micafungin 50mg/day vs. fluconazole 400mg/day vs. itraconazole 200mg/day as prophylaxis for adult patients with various haematological diseases receiving haploidentical hematopoietic stem cell transplantation (haplo-HSCT) followed by high-dose cyclophosphamide (PT-Cy). Overall, 99 patients were identified: 30 patients received micafungin, 50 and 19 patients received itraconazole and fluconazole, respectively. After a median follow-up of 12 months (range: 1-51), proven or probable IFIs were reported in 3 patients (10%) in the micafungin, 5 patients in the itraconazole (10%) and 2 patients (11%) in the fluconazole group (p=0.998). Fewer patients in the micafungin group had invasive aspergillosis (1 [3%] vs. 3 [6%] in the itraconazole vs. 2 [11%] in the fluconazole group, p=0.589). Four patients (13%) in the micafungin group vs 13 (26%) patients in the itraconazole group and 10 (53%) patients in the fluconazole received empirical antifungal therapy (P = 0.19). No serious adverse events related to treatment were reported by patients, and there was no treatment discontinuation because of drug-related adverse events in both groups. The present analysis shows that micafungin did better than fluconazole in preventing invasive aspergillosis after transplant in these high-risk hematological diseases, as expected. In addition, micafungin was more effective than itraconazole in preventing all IFI episodes when also considering possible fungal infections. Future prospective studies would shed light on this issue, concerning this increasingly used transplant platform.
在过去十年中,侵袭性真菌感染(IFI)在接受异基因造血干细胞移植(Allo-HSCT)的患者中仍然是一个重要问题。预防性抗真菌治疗的最佳方法尚未确定。我们进行了一项回顾性分析,比较了50mg/天米卡芬净与400mg/天氟康唑和200mg/天伊曲康唑作为接受单倍体造血干细胞移植(haplo-HSCT)并随后接受大剂量环磷酰胺(PT-Cy)的各种血液系统疾病成年患者预防用药的安全性和有效性。总体而言,共纳入99例患者:30例患者接受米卡芬净,50例患者接受伊曲康唑,19例患者接受氟康唑。中位随访12个月(范围:1-51个月)后,米卡芬净组有3例患者(10%)报告了确诊或疑似IFI,伊曲康唑组有5例患者(10%),氟康唑组有2例患者(11%)(p=0.998)。米卡芬净组侵袭性曲霉病患者较少(1例[3%],伊曲康唑组为3例[6%],氟康唑组为2例[11%],p=0.589)。米卡芬净组有4例患者(13%)接受了经验性抗真菌治疗,伊曲康唑组有13例((26%)患者,氟康唑组有10例(53%)患者接受了经验性抗真菌治疗(P = 0.19)。患者未报告与治疗相关的严重不良事件,两组均未因药物相关不良事件而停药。本分析表明,正如预期的那样