Reinstatler Lael, Klaassen Zachary, Barrett Brittani, Terris Martha K, Moses Kelvin A
Department of Surgery, Section of Urology, Medical College of Georgia-Georgia Regents University, Augusta, GA.
Int Braz J Urol. 2015 Jul-Aug;41(4):697-704. doi: 10.1590/S1677-5538.IBJU.2014.0383.
To explore the association of body mass index (BMI) and comorbidity with renal function after nephrectomy.
We retrospectively analyzed 263 patients submitted to partial or radical nephrectomy from 2000-2013. Variables assessed included BMI, Charlson Comorbidity Index (CCI), race, tobacco use, tumor histology, surgical approach, Fuhrman nuclear grade, and tumor (T) classification. Glomerular filtration rate (GFR) was estimated using the Cockroft-Gault equation, adjusted for gender. Logistic regression was performed and included all interaction terms.
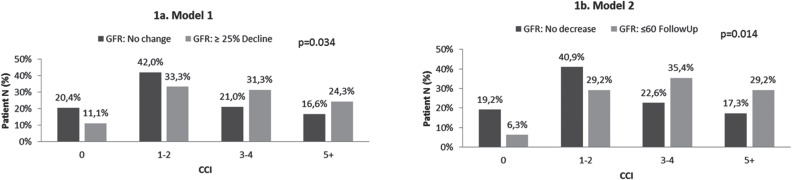
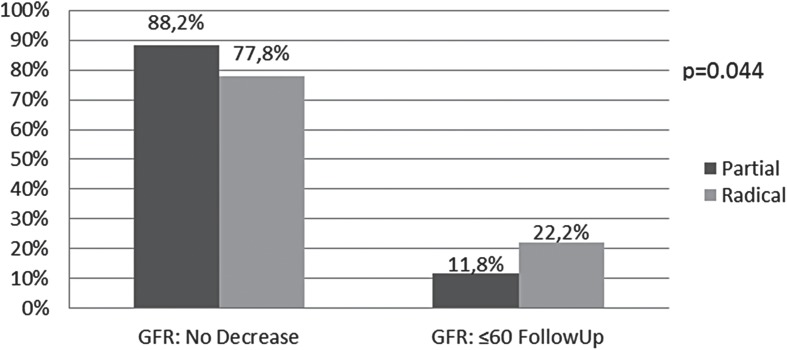
Median follow-up was 19.6 months (IQR 5.2, 53.7). Median preoperative GFR was 86.2 mL/min/1.73 m2 and median postoperative GFR was 68.4 mL/min/1.73 m2. BMI (OR 1.07, 95%CI 1.02-1.11), CCI (OR 1.19, 95%CI 1.04-1.37), and radical nephrectomy (OR 3.09, 95%CI 1.51-6.33) were significantly associated with a decline in renal function of ≥ 25%.
BMI and CCI are associated with postoperative decline in renal function after nephrectomy. Additionally, radical nephrectomy is significantly associated with decreasing renal function compared to partial nephrectomy. These findings highlight the importance of assessing patient comorbidity in the decision making process for patients presenting with a renal mass.
探讨肾切除术后体重指数(BMI)和合并症与肾功能的关系。
我们回顾性分析了2000年至2013年间接受部分或根治性肾切除术的263例患者。评估的变量包括BMI、查尔森合并症指数(CCI)、种族、吸烟情况、肿瘤组织学、手术方式、富尔曼核分级和肿瘤(T)分期。采用Cockcroft-Gault方程估算肾小球滤过率(GFR),并根据性别进行调整。进行逻辑回归分析,纳入所有交互项。
中位随访时间为19.6个月(四分位间距5.2,53.7)。术前GFR中位数为86.2 mL/min/1.73 m²,术后GFR中位数为68.4 mL/min/1.73 m²。BMI(比值比1.07,95%置信区间1.02 - 1.11)、CCI(比值比1.19,95%置信区间1.04 - 1.37)和根治性肾切除术(比值比3.09,95%置信区间1.51 - 6.33)与肾功能下降≥25%显著相关。
BMI和CCI与肾切除术后肾功能下降有关。此外,与部分肾切除术相比,根治性肾切除术与肾功能下降显著相关。这些发现凸显了在肾肿块患者的决策过程中评估患者合并症的重要性。