Aggarwal Aakash, Arora Sumant, Singh Pahul, Nat Amitpal
Aakash Aggarwal, Department of Internal Medicine,, SUNY Upstate, 750 E Adams St., 24 Presidential Court,, Syracuse, New York 13202,, United States, T: 3153910615,
Ann Saudi Med. 2015 May-Jun;35(3):257-9. doi: 10.5144/0256-4947.2015.257.
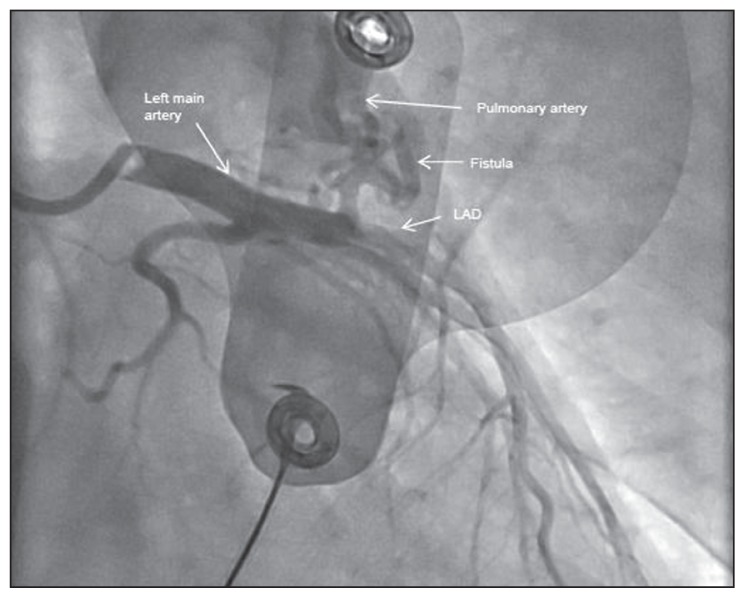
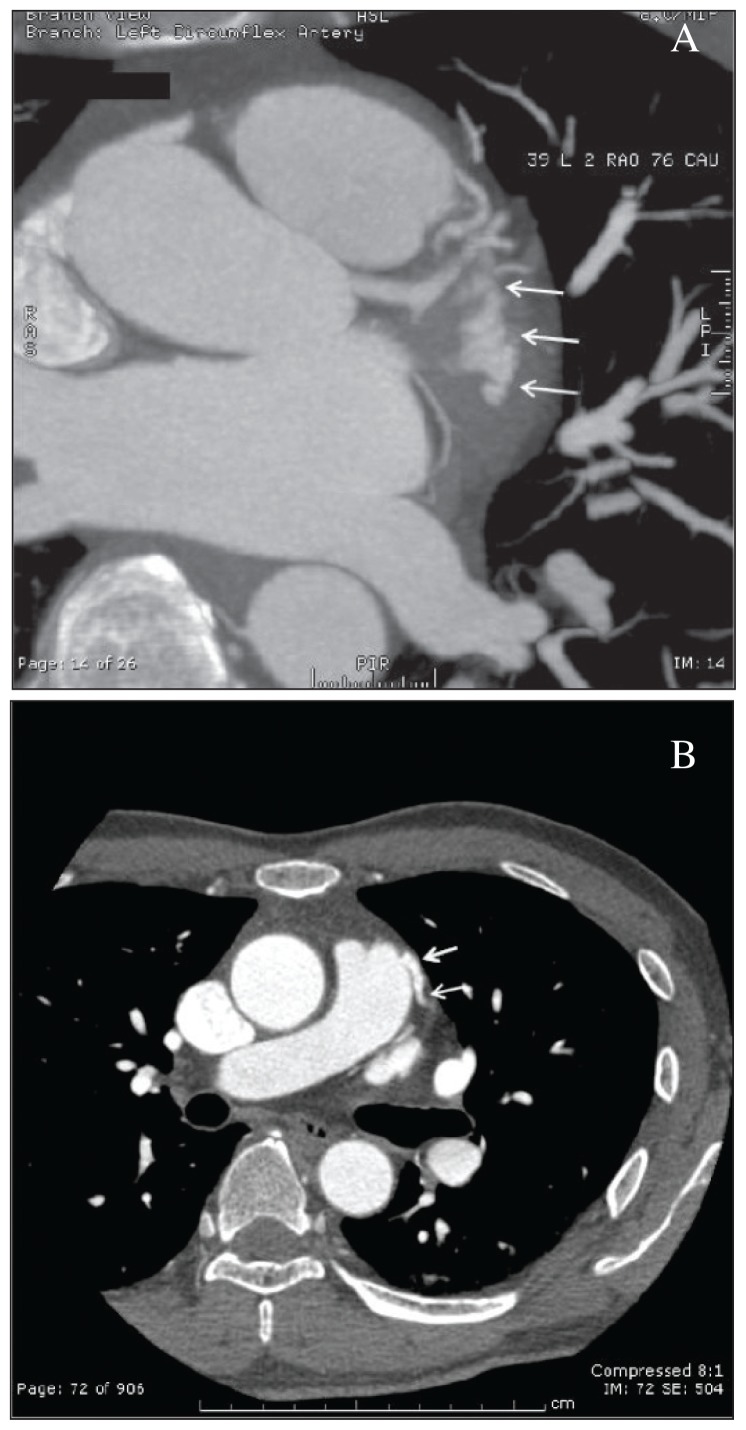
Coronary fistulas are anomalous shunts from a coronary artery to a cardiac chamber or great vessel, bypassing the myocardial circulation. A 42-year-old Asian man with no significant history of cardiac disease presented with exertional chest discomfort in the form of chest tightness over the precordial area. The patient had no cardiac risk factors, but given the duration and persistence of symptoms, we did a stress echocardiogram. The exercise led to a 'coronary artery steal phenomenon' caused by the coronary fistula, which diverted the blood from the left anterior descending artery to the pulmonary artery thereby producing the ischemic symptoms and ventricular tachycardia. Transcatheter coil embolization was unsuccessful, but the fistula was eventually closed surgically. A repeat stress echocardiogram before discharge was completely normal. We emphasize the need to individualize treatment, taking into consideration all factors in a particular patient.
冠状动脉瘘是冠状动脉与心腔或大血管之间的异常分流,绕过心肌循环。一名42岁无明显心脏病史的亚洲男性,出现劳累性胸部不适,表现为心前区胸闷。该患者无心脏危险因素,但鉴于症状的持续时间和持续性,我们进行了负荷超声心动图检查。运动导致由冠状动脉瘘引起的“冠状动脉窃血现象”,使血液从左前降支动脉分流至肺动脉,从而产生缺血症状和室性心动过速。经导管线圈栓塞术未成功,但瘘最终通过手术闭合。出院前复查的负荷超声心动图完全正常。我们强调需要个体化治疗,考虑特定患者的所有因素。