Ong David S Y, Spitoni Cristian, Klein Klouwenberg Peter M C, Verduyn Lunel Frans M, Frencken Jos F, Schultz Marcus J, van der Poll Tom, Kesecioglu Jozef, Bonten Marc J M, Cremer Olaf L
Department of Medical Microbiology, University Medical Center Utrecht, Utrecht, The Netherlands.
Department of Intensive Care Medicine, University Medical Center Utrecht, Utrecht, The Netherlands.
Intensive Care Med. 2016 Mar;42(3):333-341. doi: 10.1007/s00134-015-4071-z. Epub 2015 Sep 28.
Cytomegalovirus (CMV) reactivation occurs frequently in patients with the acute respiratory distress syndrome (ARDS) and has been associated with increased mortality. However, it remains unknown whether this association represents an independent risk for poor outcome. We aimed to estimate the attributable effect of CMV reactivation on mortality in immunocompetent ARDS patients.
We prospectively studied immunocompetent ARDS patients who tested seropositive for CMV and remained mechanically ventilated beyond day 4 in two tertiary intensive care units in the Netherlands from 2011 to 2013. CMV loads were determined in plasma weekly. Competing risks Cox regression was used with CMV reactivation status as a time-dependent exposure variable. Subsequently, in sensitivity analyses we adjusted for the evolution of disease severity until onset of reactivation using marginal structural modeling.
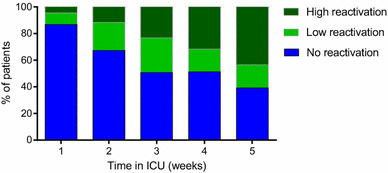
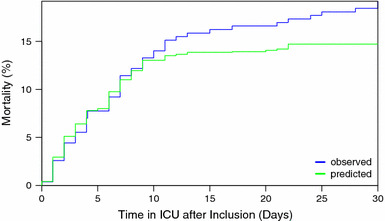
Of 399 ARDS patients, 271 (68%) were CMV seropositive and reactivation occurred in 74 (27%) of them. After adjustment for confounding and competing risks, CMV reactivation was associated with overall increased ICU mortality (adjusted subdistribution hazard ratio (SHR) 2.74, 95% CI 1.51-4.97), which resulted from the joint action of trends toward an increased mortality rate (direct effect; cause specific hazard ratio (HR) 1.58, 95% CI 0.86-2.90) and a reduced successful weaning rate (indirect effect; cause specific HR 0.83, 95% CI 0.58-1.18). These associations remained in sensitivity analyses. The population-attributable fraction of ICU mortality was 23% (95% CI 6-41) by day 30 (risk difference 4.4, 95% CI 1.1-7.9).
CMV reactivation is independently associated with increased case fatality in immunocompetent ARDS patients who are CMV seropositive.
巨细胞病毒(CMV)再激活在急性呼吸窘迫综合征(ARDS)患者中频繁发生,且与死亡率增加相关。然而,这种关联是否代表不良预后的独立风险仍不清楚。我们旨在评估CMV再激活对免疫功能正常的ARDS患者死亡率的归因效应。
我们对2011年至2013年在荷兰两家三级重症监护病房中CMV血清学检测呈阳性且机械通气超过4天的免疫功能正常的ARDS患者进行了前瞻性研究。每周测定血浆中的CMV载量。采用竞争风险Cox回归,将CMV再激活状态作为时间依赖性暴露变量。随后,在敏感性分析中,我们使用边际结构模型对再激活开始前疾病严重程度的演变进行了调整。
在399例ARDS患者中,271例(68%)CMV血清学呈阳性,其中74例(27%)发生了再激活。在调整混杂因素和竞争风险后,CMV再激活与ICU总体死亡率增加相关(调整后的亚分布风险比(SHR)为2.74,95%置信区间为1.51 - 4.97),这是死亡率上升趋势(直接效应;病因特异性风险比(HR)为1.58,95%置信区间为0.86 - 2.90)和成功脱机率降低(间接效应;病因特异性HR为0.83,95%置信区间为0.58 - 1.18)共同作用的结果。这些关联在敏感性分析中仍然存在。到第30天时,ICU死亡率的人群归因分数为23%(95%置信区间为6 - 41)(风险差异为4.4,95%置信区间为1.1 - 7.9)。
CMV再激活与CMV血清学呈阳性的免疫功能正常的ARDS患者病死率增加独立相关。