Kotecha Dipak, Piccini Jonathan P
Institute of Cardiovascular Science, University of Birmingham, Birmingham, UK Monash Centre of Cardiovascular Research and Education in Therapeutics, Monash University, Melbourne, Australia
Duke Center for Atrial Fibrillation, Clinical Cardiac Electrophysiology, Duke University Medical Center, Durham, USA.
Eur Heart J. 2015 Dec 7;36(46):3250-7. doi: 10.1093/eurheartj/ehv513. Epub 2015 Sep 28.
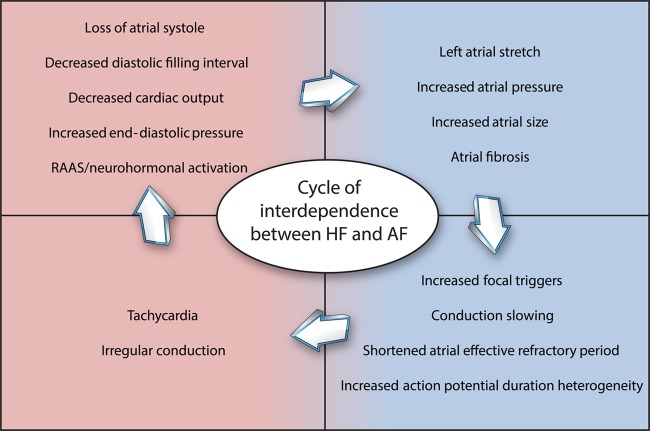
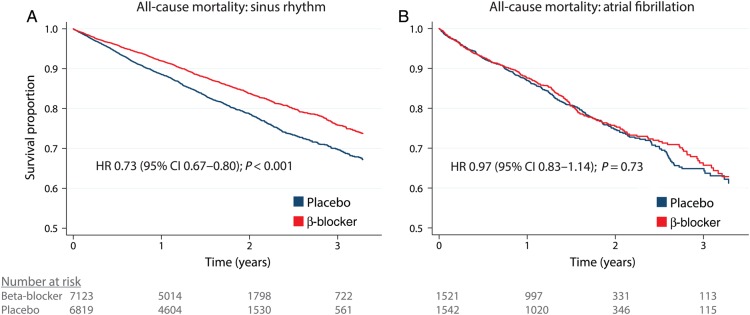
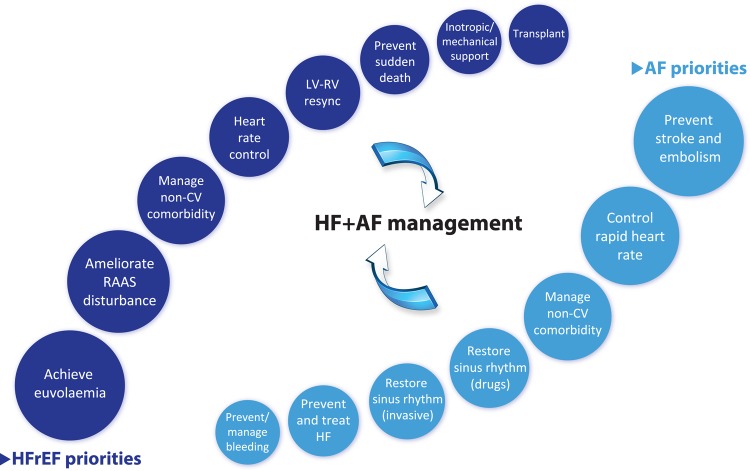
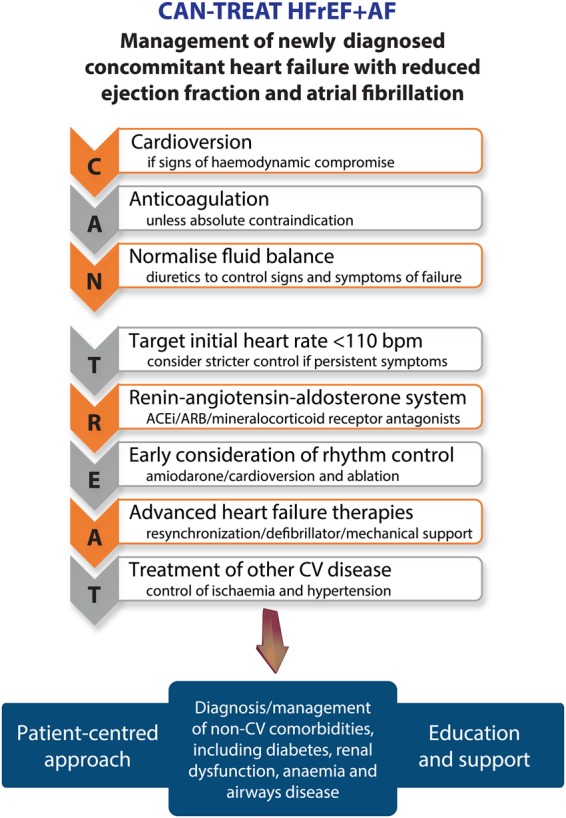
Heart failure (HF) and atrial fibrillation (AF) are two conditions that are likely to dominate the next 50 years of cardiovascular (CV) care. Both are increasingly prevalent and associated with high morbidity, mortality, and healthcare cost. They are closely inter-related with similar risk factors and shared pathophysiology. Patients with concomitant HF and AF suffer from even worse symptoms and poorer prognosis, yet evidence-based evaluation and management of this group of patients is lacking. In this review, we evaluate the common mechanisms for the development of AF in HF patients and vice versa, focusing on the evidence for potential treatment strategies. Recent data have suggested that these patients may respond differently than those with HF or AF alone. These results highlight the clear clinical need to identify and treat according to best evidence, in order to prevent adverse outcomes and reduce the huge burden that HF and AF are expected to have on global healthcare systems in the future. We propose an easy-to-use clinical mnemonic to aid the initial management of newly discovered concomitant HF and AF, the CAN-TREAT HFrEF + AF algorithm (Cardioversion if compromised; Anticoagulation unless contraindication; Normalize fluid balance; Target initial heart rate <110 b.p.m.; Renin-angiotensin-aldosterone modification; Early consideration of rhythm control; Advanced HF therapies; Treatment of other CV disease).
心力衰竭(HF)和心房颤动(AF)是未来50年心血管(CV)护理中可能占据主导地位的两种疾病。二者都日益普遍,且与高发病率、高死亡率及高昂的医疗费用相关。它们密切相关,具有相似的危险因素和共同的病理生理学机制。合并HF和AF的患者症状更严重,预后更差,但针对这组患者的循证评估和管理却很缺乏。在本综述中,我们评估了HF患者发生AF及反之亦然的常见机制,重点关注潜在治疗策略的证据。近期数据表明,这些患者的反应可能与单纯患有HF或AF的患者不同。这些结果凸显了根据最佳证据进行识别和治疗的明确临床需求,以预防不良后果,并减轻HF和AF未来预计会给全球医疗系统带来的巨大负担。我们提出了一种易于使用的临床记忆方法,以辅助新发现的合并HF和AF患者的初始管理,即CAN-TREAT HFrEF + AF算法(若情况不佳则进行复律;若无禁忌则进行抗凝;使液体平衡正常化;将初始心率目标设定为<110次/分钟;调整肾素-血管紧张素-醛固酮系统;尽早考虑节律控制;采用晚期HF治疗方法;治疗其他CV疾病)。