Friedrich Paola, Lam Catherine G, Itriago Elena, Perez Rafael, Ribeiro Raul C, Arora Ramandeep S
Department of Pediatric Oncology, Dana-Farber/Boston Children's Cancer and Blood Disorders Center, Boston, Massachusetts, United States of America.
Department of Oncology, St. Jude Children's Research Hospital, Memphis, Tennessee, United States of America; International Outreach Program, St. Jude Children's Research Hospital, Memphis, Tennessee, United States of America.
PLoS One. 2015 Sep 30;10(9):e0135230. doi: 10.1371/journal.pone.0135230. eCollection 2015.
Treatment abandonment (TxA) is recognized as a leading cause of treatment failure for children with cancer in low-and-middle-income countries (LMC). However, its global frequency and burden have remained elusive due to lack of global data. This study aimed to obtain an estimate using survey and population data.
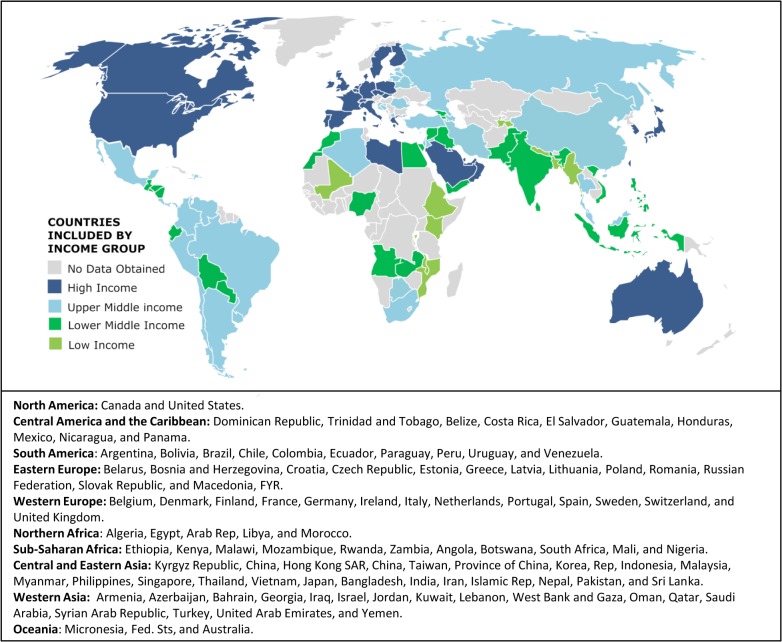
Childhood cancer clinicians (medical oncologists, surgeons, and radiation therapists), nurses, social workers, and psychologists involved in care of children with cancer were approached through an online survey February-May 2012. Incidence and population data were obtained from public sources. Descriptive, univariable, and multivariable analyses were conducted.
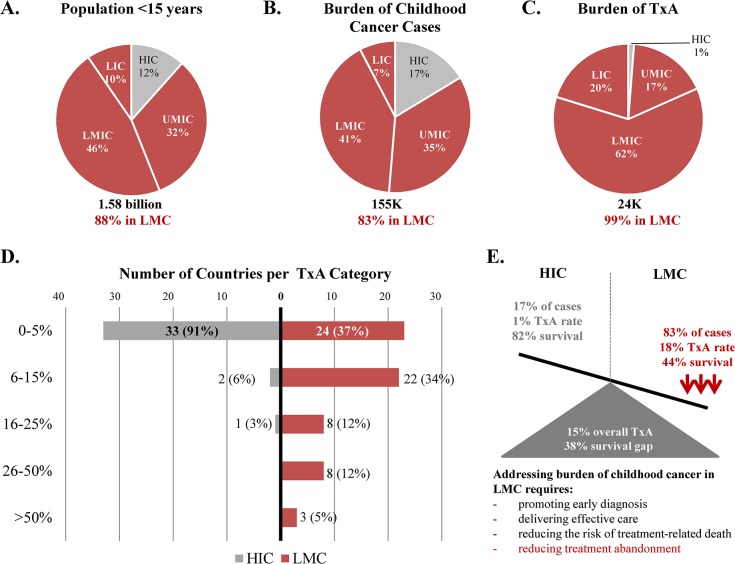
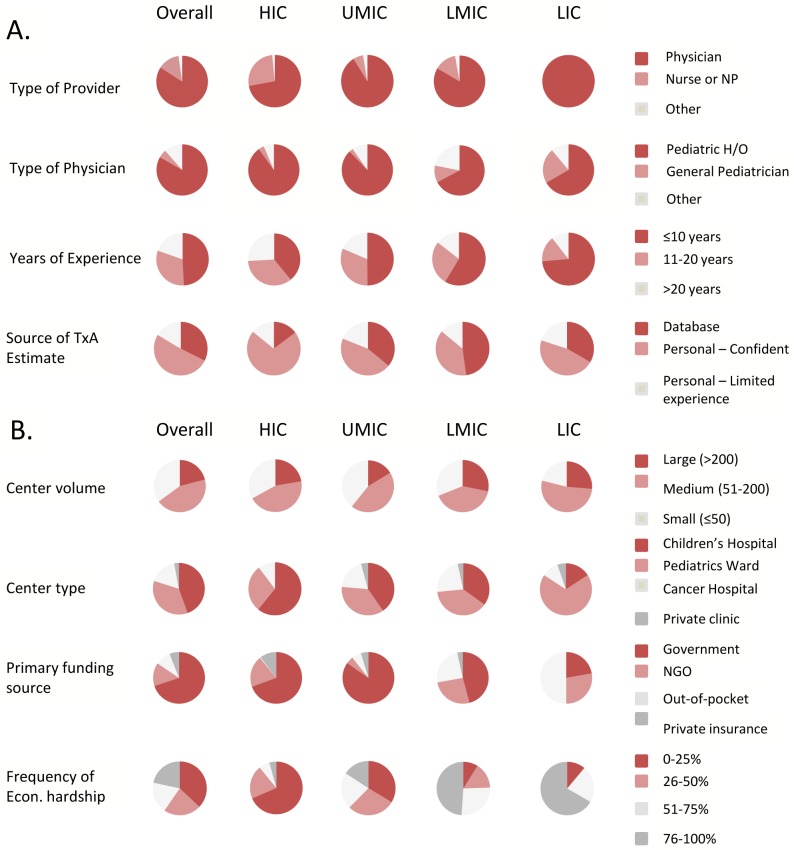
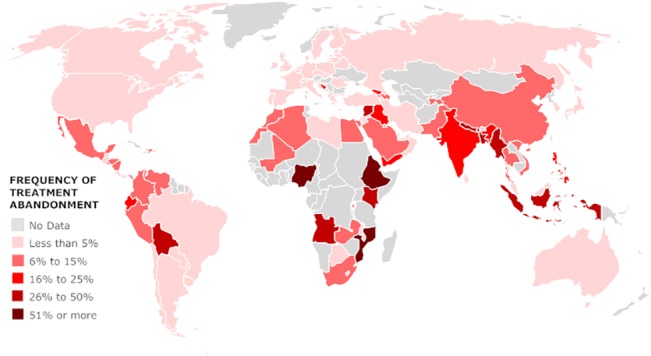
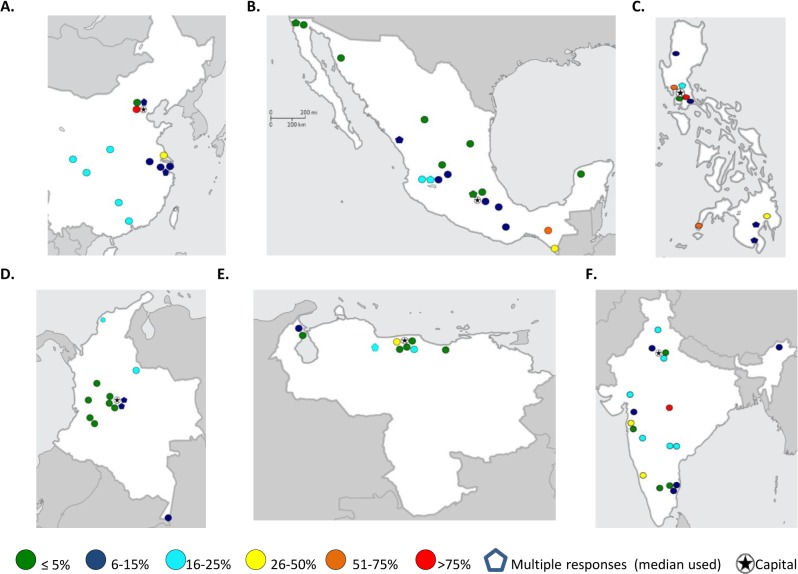
602 responses from 101 countries were obtained from physicians (84%), practicing pediatric hematology/oncology (83%) in general or children's hospitals (79%). Results suggested, 23,854 (15%) of 155,088 children <15 years old newly diagnosed with cancer annually in the countries analyzed, abandon therapy. Importantly, 83% of new childhood cancer cases and 99% of TxA were attributable to LMC. The annual number of cases of TxA expected in LMC worldwide (26,166) was nearly equivalent to the annual number of cancer cases in children <15 years expected in HIC (26,368). Approximately two thirds of LMC had median TxA ≥ 6%, but TxA ≥ 6% was reported in high- (9%), upper-middle- (41%), lower-middle- (80%), and low-income countries (90%, p<0.001). Most LMC centers reporting TxA > 6% were outside the capital. Lower national income category, higher reliance on out-of-pocket payments, and high prevalence of economic hardship at the center were independent contextual predictors for TxA ≥ 6% (p<0.001). Global survival data available for more developed and less developed regions suggests TxA may account for at least a third of the survival gap between HIC and LMC.
Results show TxA is prevalent (compromising cancer survival for 1 in 7 children globally), confirm the suspected high burden of TxA in LMC, and illustrate the negative impact of poverty on its occurrence. The present estimates may appear small compared to the global burden of child death from malnutrition and infection (measured in millions). However, absolute numbers suggest the burden of TxA in LMC is nearly equivalent to annually losing all kids diagnosed with cancer in HIC just to TxA, without even considering deaths from disease progression, relapse or toxicity-the main causes of childhood cancer mortality in HIC. Results document the importance of monitoring and addressing TxA as part of childhood cancer outcomes in at-risk settings.
治疗放弃(TxA)被认为是低收入和中等收入国家(LMC)儿童癌症治疗失败的主要原因。然而,由于缺乏全球数据,其全球发生率和负担仍不明确。本研究旨在利用调查和人口数据进行估算。
2012年2月至5月,通过在线调查联系了参与儿童癌症护理的儿童癌症临床医生(医学肿瘤学家、外科医生和放射治疗师)、护士、社会工作者和心理学家。发病率和人口数据来自公共来源。进行了描述性、单变量和多变量分析。
从101个国家获得了602份回复,回复者为医生(84%),在综合医院或儿童医院从事儿科血液学/肿瘤学工作(83%)。结果表明,在分析的国家中,每年新诊断的155,088名15岁以下儿童中有23,854名(15%)放弃治疗。重要的是,83%的儿童癌症新病例和99%的治疗放弃病例归因于低收入和中等收入国家。全球低收入和中等收入国家预计的每年治疗放弃病例数(26,166例)几乎等同于高收入国家预计的每年15岁以下儿童癌症病例数(26,368例)。大约三分之二的低收入和中等收入国家治疗放弃率中位数≥6%,但高收入国家(9%)、中高收入国家(41%)、中低收入国家(80%)和低收入国家(90%,p<0.001)均报告有治疗放弃率≥6%的情况。报告治疗放弃率>6%的大多数低收入和中等收入国家中心位于首都以外。较低的国民收入类别、对自费支付的更高依赖以及中心经济困难的高流行率是治疗放弃率≥6%的独立背景预测因素(p<0.001)。可用于更发达和欠发达地区的全球生存数据表明,治疗放弃可能至少占高收入国家和低收入和中等收入国家之间生存差距的三分之一。
结果表明治疗放弃很普遍(全球每7名儿童中就有1名的癌症生存受到影响),证实了低收入和中等收入国家治疗放弃负担高的怀疑,并说明了贫困对其发生的负面影响。与全球营养不良和感染导致的儿童死亡负担(以数百万计)相比,目前的估算数字可能看起来较小。然而,绝对数字表明,低收入和中等收入国家治疗放弃的负担几乎等同于每年仅因治疗放弃就失去高收入国家所有被诊断患有癌症的儿童,甚至不考虑疾病进展、复发或毒性导致的死亡——高收入国家儿童癌症死亡的主要原因。结果证明了在高危环境中监测和解决治疗放弃问题作为儿童癌症治疗结果一部分的重要性。