Saunders Erika Fh, Reider Aubrey, Singh Gagan, Gelenberg Alan J, Rapoport Stanley I
Department of Psychiatry, Penn State College of Medicine, Penn State Milton S. Hershey Medical Center, Hershey, PA, USA.
University of Michigan Department of Psychiatry, Ann Arbor, MI, USA.
Bipolar Disord. 2015 Nov;17(7):729-42. doi: 10.1111/bdi.12337. Epub 2015 Oct 1.
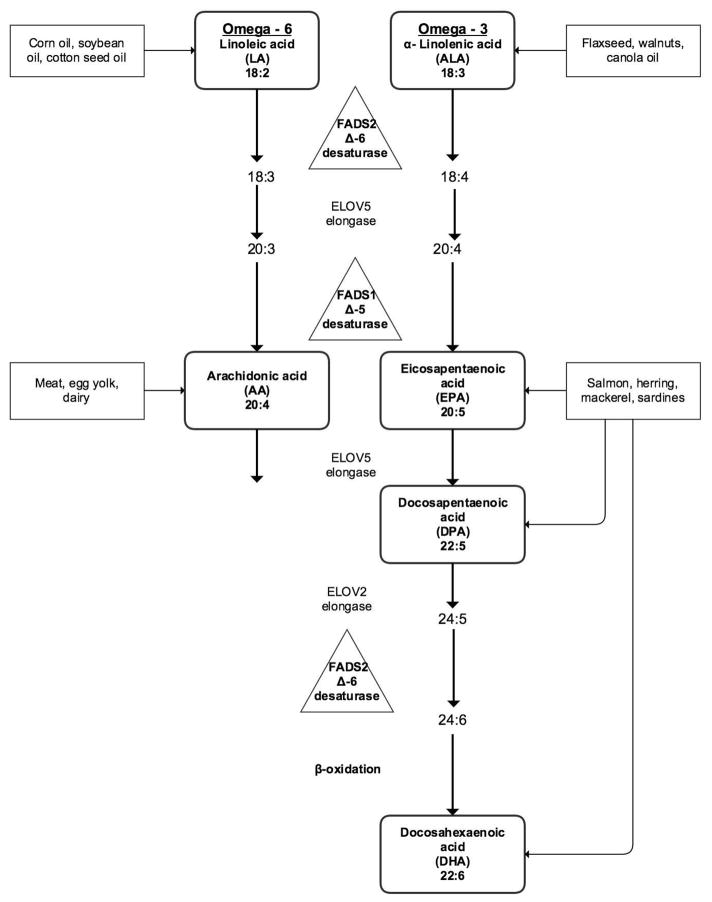
Omega (n)-3 and n-6 polyunsaturated fatty acids (PUFAs) are molecular modulators of neurotransmission and inflammation. We hypothesized that plasma concentrations of n-3 PUFAs would be lower and those of n-6 PUFAs higher in subjects with bipolar disorder (BD) compared to healthy controls (HCs), and would correlate with symptom severity in subjects with BD, and that effective treatment would correlate with increased n-3 but lower n-6 PUFA levels. Additionally, we explored clinical correlations and group differences in plasma levels of saturated and monounsaturated fatty acids.
This observational, parallel group study compared biomarkers between HCs (n = 31) and symptomatic subjects with BD (n = 27) when ill and after symptomatic recovery (follow-up). Plasma concentrations of five PUFAs [linoleic acid (LA), arachidonic acid (AA), alpha-linolenic acid (ALA), docosahexaenoic acid (DHA), and eicosapentaenoic acid (EPA)], two saturated fatty acids (palmitic acid and stearic acid) and two monounsaturated fatty acids (palmitoleic acid and oleic acid) were measured in esterified (E) and unesterified (UE) forms. Calculated ratios included UE:E for the five PUFAs, ratios of n-3 PUFAs (DHA:ALA, EPA:ALA and EPA:DHA), and the ratio of n-6:n-3 AA:EPA. Comparisons of plasma fatty acid levels and ratios between BD and HC groups were made with Student t-tests, and between the BD group at baseline and follow-up using paired t-tests. Comparison of categorical variables was performed using chi-square tests. Pearson's r was used for bivariate correlations with clinical variables, including depressive and manic symptoms, current panic attacks, and psychosis.
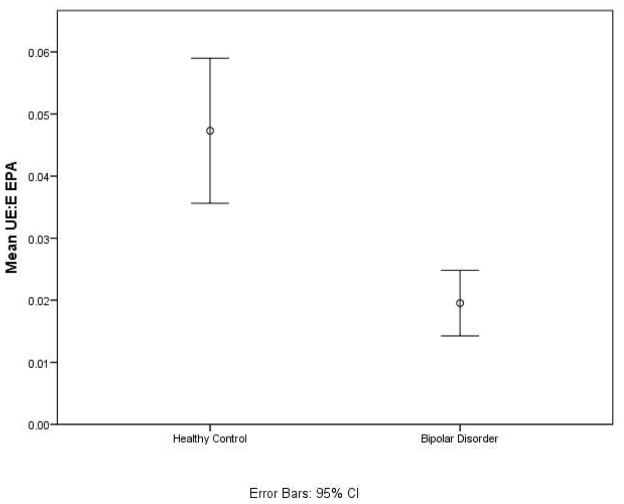
UE EPA was lower in subjects with BD than in HCs, with a large effect size (Cohen's d = 0.86, p < 0.002); however, it was not statistically significant after correction for multiple comparisons. No statistically significant difference was seen in any plasma PUFA concentration between the BD and HC groups after Bonferroni correction for 40 comparisons, at p < 0.001. Neither depressive severity nor mania severity was correlated significantly with any PUFA concentration. Exploratory comparison showed lower UE:E EPA in the BD than the HC group (p < 0.0001). At follow-up in the BD group, UE, E DHA:ALA, and UE EPA:ALA were decreased (p < 0.002). Exploratory correlations of clinical variables revealed that mania severity and suicidality were positively correlated with UE:E EPA ratio, and that several plasma levels and ratios correlated with panic disorder and psychosis. Depressive severity was not correlated with any ratio. No plasma fatty acid level or ratio correlated with self-reported n-3 PUFA intake or use of medication by class.
A large effect size of reduced UE EPA, and a lower plasma UE:E concentration ratio of EPA in the symptomatic BD state may be important factors in vulnerability to a mood state. Altered n-3 PUFA ratios could indicate changes in PUFA metabolism concurrent with symptom improvement. Our findings are consistent with preclinical and postmortem data and suggest testing interventions that increase n-3 and decrease n-6 dietary PUFA intake.
ω-3和ω-6多不饱和脂肪酸(PUFAs)是神经传递和炎症的分子调节剂。我们假设,与健康对照者(HCs)相比,双相情感障碍(BD)患者血浆中ω-3多不饱和脂肪酸的浓度会更低,而ω-6多不饱和脂肪酸的浓度会更高,且这与BD患者的症状严重程度相关,有效治疗会与ω-3多不饱和脂肪酸水平升高但ω-6多不饱和脂肪酸水平降低相关。此外,我们还探讨了饱和脂肪酸和单不饱和脂肪酸血浆水平的临床相关性及组间差异。
这项观察性平行组研究比较了HCs(n = 31)与有症状的BD患者(n = 27)在患病时及症状缓解后(随访)的生物标志物。测定了五种PUFAs[亚油酸(LA)、花生四烯酸(AA)、α-亚麻酸(ALA)、二十二碳六烯酸(DHA)和二十碳五烯酸(EPA)]、两种饱和脂肪酸(棕榈酸和硬脂酸)以及两种单不饱和脂肪酸(棕榈油酸和油酸)的酯化(E)和非酯化(UE)形式的血浆浓度。计算的比值包括五种PUFAs的UE:E、ω-3多不饱和脂肪酸的比值(DHA:ALA、EPA:ALA和EPA:DHA)以及ω-6:ω-3 AA:EPA的比值。使用Student t检验比较BD组和HC组之间的血浆脂肪酸水平及比值,使用配对t检验比较BD组基线和随访时的情况。使用卡方检验进行分类变量的比较。Pearson相关系数r用于与临床变量进行双变量相关分析,包括抑郁和躁狂症状、当前惊恐发作和精神病。
BD患者的非酯化EPA低于HCs,效应量较大(Cohen's d = 0.86,p < 0.002);然而,在进行多重比较校正后,差异无统计学意义。在对40次比较进行Bonferroni校正后,p < 0.001时,BD组和HC组之间的任何血浆PUFA浓度均无统计学显著差异。抑郁严重程度和躁狂严重程度与任何PUFA浓度均无显著相关性。探索性比较显示,BD组的非酯化:酯化EPA低于HC组(p < 0.0001)。在BD组随访时,非酯化、酯化DHA:ALA以及非酯化EPA:ALA均降低(p < 0.002)。临床变量的探索性相关分析显示,躁狂严重程度和自杀倾向与非酯化:酯化EPA比值呈正相关,且几种血浆水平和比值与惊恐障碍和精神病相关。抑郁严重程度与任何比值均无相关性。没有血浆脂肪酸水平或比值与自我报告的ω-3多不饱和脂肪酸摄入量或按类别使用的药物相关。
非酯化EPA降低的效应量较大,且有症状的BD状态下血浆非酯化:酯化EPA浓度比值较低可能是易患情绪状态的重要因素。ω-3多不饱和脂肪酸比值的改变可能表明PUFA代谢的变化与症状改善同时发生。我们的研究结果与临床前和尸检数据一致,并建议测试增加ω-3和减少ω-6膳食PUFA摄入量的干预措施。