Wang Jing, Zhou Min, Xu Jing-Yan, Chen Bing, Ouyang Jian
Department of Hematology, The Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, Jiangsu, People's Republic of China.
Onco Targets Ther. 2015 Sep 18;8:2645-50. doi: 10.2147/OTT.S86093. eCollection 2015.
To evaluate whether the addition of two biological markers (MYC and BCL-2 protein overexpression) improves the stratification of high-risk patients with diffuse large B-cell lymphoma (DLBCL).
Seven risk factors were identified at diagnosis, and a maximum of 7 points were assigned to each patient. The patients were classified according to four risk groups: low (0-1), low-intermediate (2-3), high-intermediate (4), and high (5-7). Only high-risk patients with DLBCL were included in this analysis. We retrospectively examined 20 cases from 2008 to 2013 at the Nanjing Drum Tower Hospital.
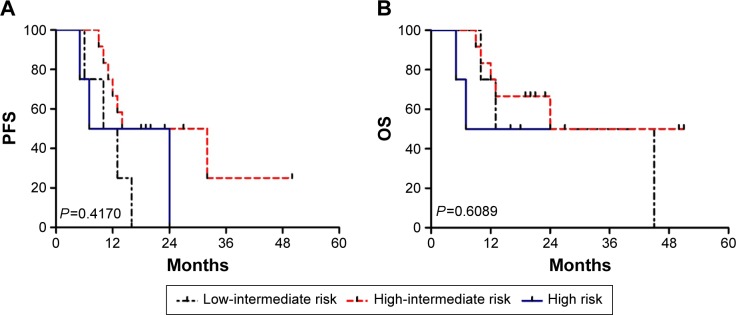
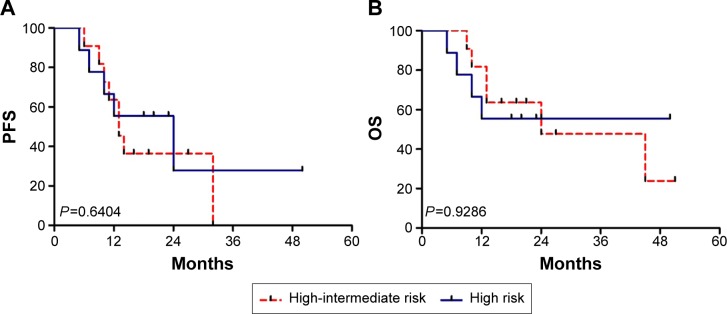
The median expression of MYC protein was 60%, and 17 of 20 (65%) evaluable cases overexpressed MYC. The median expression of BCL-2 protein was also 60%. Eighteen of 20 (90%) evaluable cases showed BCL-2 overexpression. Additionally, 12 out of 20 cases (60%) demonstrated coexpression of MYC and BCL-2 proteins. The percentages of overall survival and progression-free survival at the median follow-up time (36 months) were 33.3%±16.1% and 16.9%±13.5%, respectively. By comparison, nine, four, and 20 patients were classified as high risk based on the International Prognostic Index (IPI), National Comprehensive Cancer Network(NCCN)-IPI, and revised IPI criteria, respectively. According to the IPI and NCCN-IPI stratification, the risk groups demonstrated closely overlapping survival curves. In addition, four out of 20 cases were identified as low-intermediate risk according to the NCCN-IPI criteria.
The addition of MYC and BCL-2 protein expression to the IPI could identify a subset of DLBCL patients with high-risk clinicopathological characteristics and poor clinical outcome.
评估添加两种生物标志物(MYC和BCL-2蛋白过表达)是否能改善弥漫性大B细胞淋巴瘤(DLBCL)高危患者的分层。
诊断时确定了7个风险因素,每位患者最多可获得7分。患者根据四个风险组进行分类:低风险(0-1分)、低中风险(2-3分)、高中风险(4分)和高风险(5-7分)。本分析仅纳入DLBCL高危患者。我们回顾性研究了南京鼓楼医院2008年至2013年的20例病例。
MYC蛋白的中位表达率为60%,20例可评估病例中有17例(65%)MYC过表达。BCL-2蛋白的中位表达率也为60%。20例可评估病例中有18例(90%)显示BCL-2过表达。此外,20例病例中有12例(60%)显示MYC和BCL-2蛋白共表达。中位随访时间(36个月)时的总生存率和无进展生存率分别为33.3%±16.1%和16.9%±13.5%。相比之下,根据国际预后指数(IPI)、美国国立综合癌症网络(NCCN)-IPI和修订后的IPI标准,分别有9例、4例和20例患者被归类为高风险。根据IPI和NCCN-IPI分层,风险组的生存曲线紧密重叠。此外,根据NCCN-IPI标准,20例病例中有4例被确定为低中风险。
在IPI中添加MYC和BCL-2蛋白表达可识别出一部分具有高危临床病理特征和不良临床结局的DLBCL患者。