Boyles Tom H, Davis Kelly, Crede Thomas, Malan Jacques, Mendelson Marc, Lesosky Maia
Division of Infectious Diseases and HIV Medicine, Department of Medicine, Groote Schuur Hospital, University of Cape Town, Observatory, 7925, Cape Town, South Africa.
University of Texas Southwestern Medical Center, Dallas, TX, USA.
BMC Infect Dis. 2015 Oct 6;15:410. doi: 10.1186/s12879-015-1127-1.
Febrile illness with suspected blood stream infection (BSI) is a common reason for admission to hospital in Africa and blood cultures are therefore an important investigation. Data on the prevalence and causes of community acquired BSI in Africa are scarce and there are no studies from South Africa. There are no validated clinical prediction rules for use of blood cultures in Africa.
A prospective observational cohort study of patients attending 2 urban emergency departments in Cape Town, South Africa. The decision to take a blood culture was made by the attending clinician and information available at the time of blood draw was collected. Bottles were weighed to measure volume of blood inoculated.
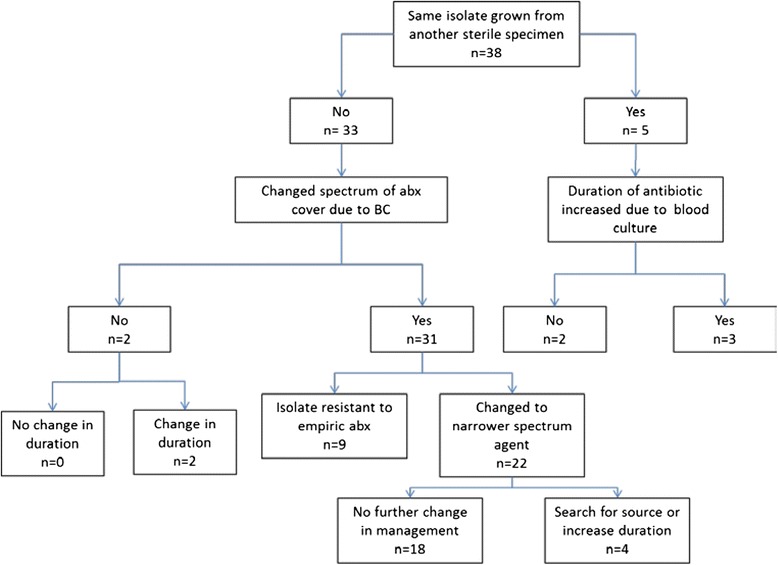
500 blood culture sets were obtained from 489 patients. 39 (7.8 %) were positive for pathogens and 13 (2.6 %) for contaminants. Significant independent predictors of positive cultures were diastolic blood pressure <60 mmHg, pulse >120 bpm, diabetes and a suspected biliary source of infection, but not HIV infection. Positive results influenced patient management in 36 of 38 (95 %) cases with the organism being resistant to the chosen empiric antibiotic in 9 of 38 (24 %). Taking <8 ml of blood was predictive of a negative culture. The best clinical prediction rule had a negative predictive value (NPV) of 92 % which is unlikely to be high enough to be clinically useful.
Blood cultures taken from patients attending emergency departments in a high HIV prevalent city in South Africa are frequently positive and almost always influence patient management. At least 8 ml of blood should be inoculated into each bottle.
Blood cultures should be taken from all patients attending EDs in South Africa suspected of having BSI particularly if diabetic, with hypotension, tachycardia or if biliary sepsis is suspected.
疑似血流感染(BSI)的发热性疾病是非洲患者住院的常见原因,因此血培养是一项重要的检查。非洲社区获得性BSI的患病率和病因数据稀缺,南非尚无相关研究。在非洲,尚无经过验证的用于指导血培养的临床预测规则。
对南非开普敦两家城市急诊科的患者进行前瞻性观察队列研究。血培养的决定由主治医生做出,并收集采血时可获得的信息。对血培养瓶称重以测量接种的血量。
从489名患者中获取了500套血培养标本。39份(7.8%)病原体培养阳性,13份(2.6%)污染菌培养阳性。培养阳性的显著独立预测因素为舒张压<60 mmHg、脉搏>120次/分、糖尿病和疑似胆源性感染源,但不包括HIV感染。38例中有36例(95%)的阳性结果影响了患者的治疗,其中38例中有9例(约24%)的病原体对选用的经验性抗生素耐药。采血<8 ml提示培养结果为阴性。最佳临床预测规则的阴性预测值(NPV)为92%,可能不足以在临床上发挥作用。
在南非一个HIV高流行城市的急诊科患者中进行的血培养结果常常呈阳性,且几乎总是会影响患者的治疗。每个血培养瓶应接种至少8 ml血液。
南非所有疑似患有BSI的急诊科患者均应进行血培养,尤其是糖尿病患者、伴有低血压或心动过速者或疑似胆源性败血症患者。