Department of Neurology, Inje University Ilsan Paik Hospital, Goyang, Korea.
Clinical Research Center, Asan Medical Center, Seoul, Korea.
J Stroke. 2015 Sep;17(3):282-301. doi: 10.5853/jos.2015.17.3.282. Epub 2015 Sep 30.
Statins have pleiotropic effects of potential neuroprotection. However, because of lack of large randomized clinical trials, current guidelines do not provide specific recommendations on statin initiation in acute ischemic stroke (AIS). The current study aims to systematically review the statin effect in AIS.
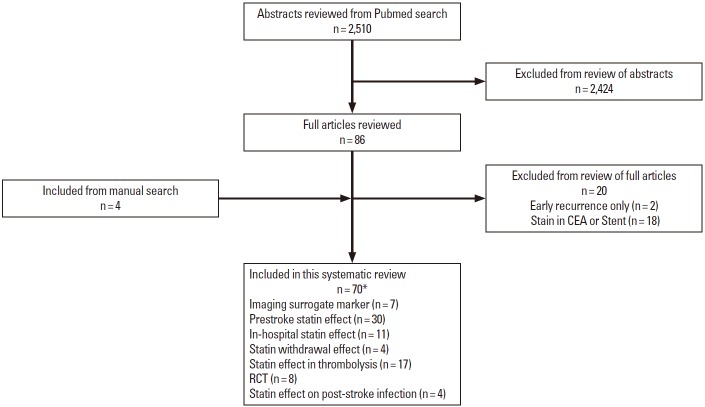
From literature review, we identified articles exploring prestroke and immediate post-stroke statin effect on imaging surrogate markers, initial stroke severity, functional outcome, and short-term mortality in human AIS. We summarized descriptive overview. In addition, for subjects with available data from publications, we conducted meta-analysis to provide pooled estimates.
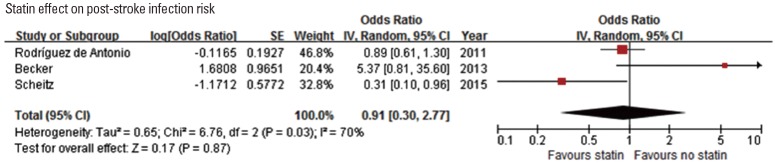
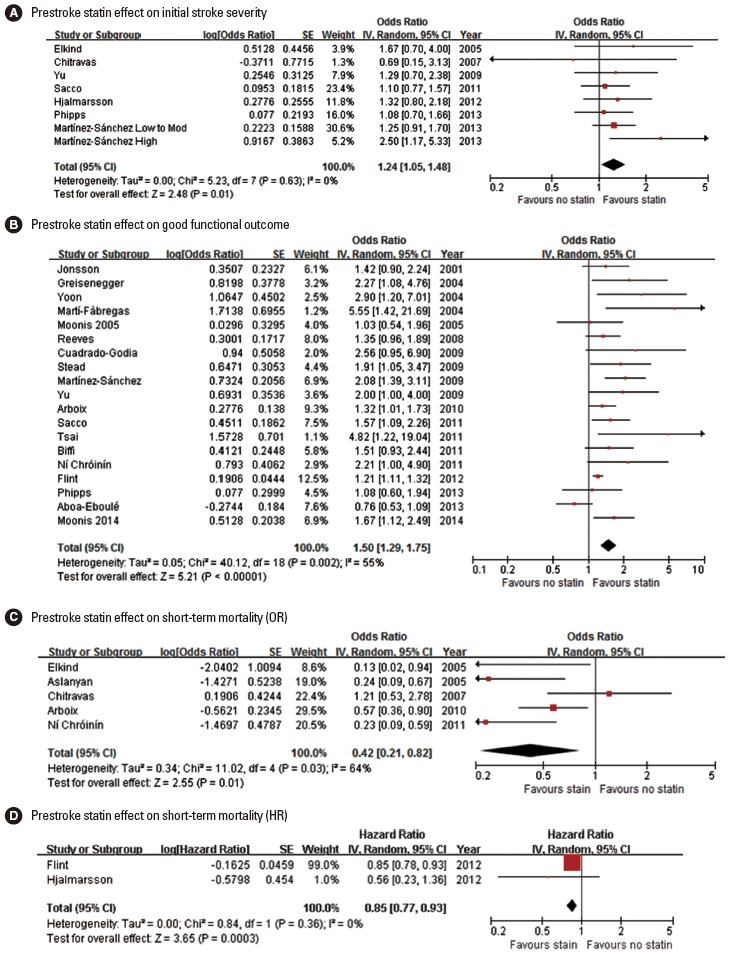
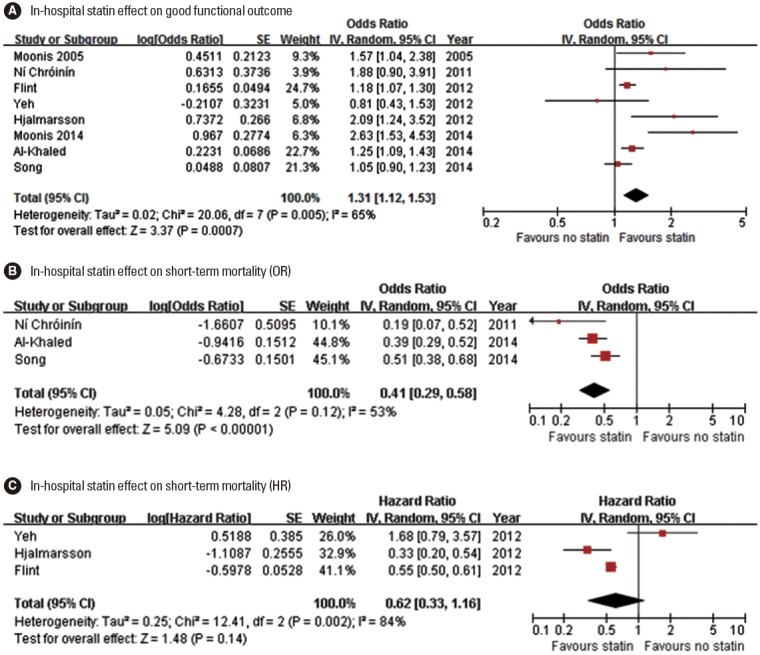
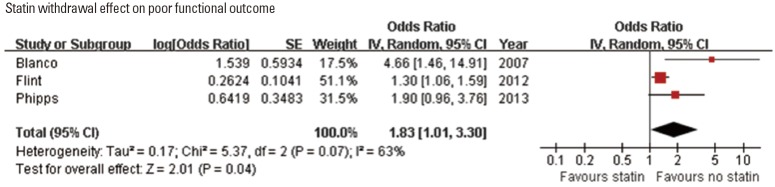
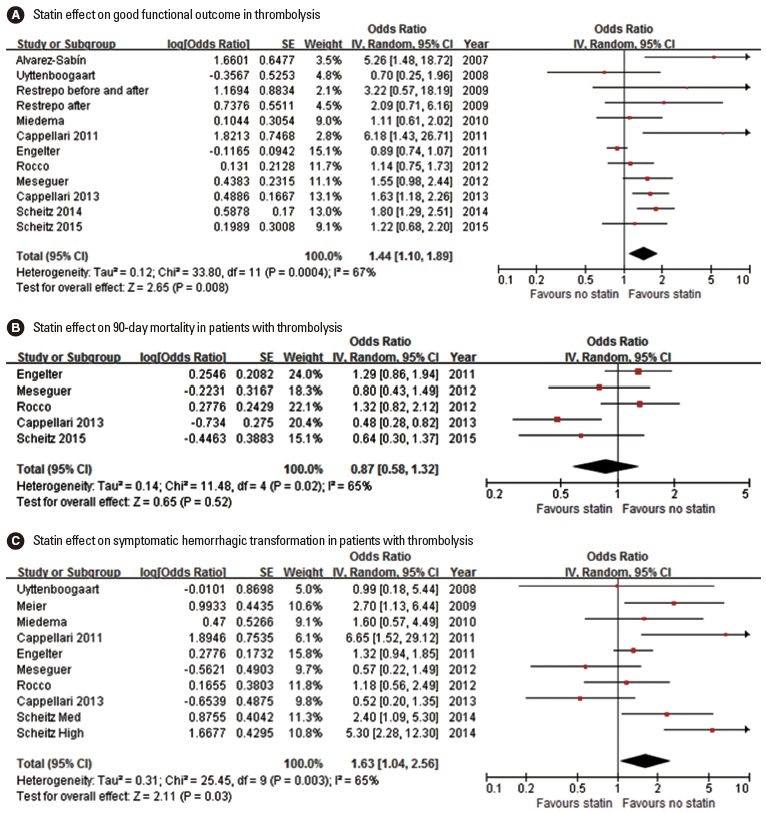
In total, we identified 70 relevant articles including 6 meta-analyses. Surrogate imaging marker studies suggested that statin might enhance collaterals and reperfusion. Our updated meta-analysis indicated that prestroke statin use was associated with milder initial stroke severity (odds ratio [OR] [95% confidence interval], 1.24 [1.05-1.48]; P=0.013), good functional outcome (1.50 [1.29-1.75]; P<0.001), and lower mortality (0.42 [0.21-0.82]; P=0.0108). In-hospital statin use was associated with good functional outcome (1.31 [1.12-1.53]; P=0.001), and lower mortality (0.41 [0.29-0.58]; P<0.001). In contrast, statin withdrawal was associated with poor functional outcome (1.83 [1.01-3.30]; P=0.045). In patients treated with thrombolysis, statin was associated with good functional outcome (1.44 [1.10-1.89]; P=0.001), despite an increased risk of symptomatic hemorrhagic transformation (1.63 [1.04-2.56]; P=0.035).
The current study findings support the use of statin in AIS. However, the findings were mostly driven by observational studies at risk of bias, and thereby large randomized clinical trials would provide confirmatory evidence.
他汀类药物具有潜在的神经保护作用。然而,由于缺乏大规模的随机临床试验,目前的指南并未就急性缺血性脑卒中(AIS)患者开始使用他汀类药物提供具体建议。本研究旨在系统地综述他汀类药物在 AIS 中的作用。
通过文献回顾,我们确定了探讨缺血前和急性脑卒中后他汀类药物对影像学替代标志物、初始脑卒中严重程度、功能结局和短期死亡率影响的研究。我们总结了描述性概述。此外,对于来自出版物的有可用数据的受试者,我们进行了荟萃分析以提供汇总估计值。
我们共确定了 70 篇相关文章,包括 6 项荟萃分析。替代影像学标志物研究表明,他汀类药物可能增强侧支循环和再灌注。我们的更新荟萃分析表明,缺血前使用他汀类药物与初始脑卒中严重程度较轻相关(比值比[OR] [95%置信区间],1.24 [1.05-1.48];P=0.013)、功能结局良好(1.50 [1.29-1.75];P<0.001)和死亡率较低(0.42 [0.21-0.82];P=0.0108)。住院期间使用他汀类药物与良好的功能结局相关(1.31 [1.12-1.53];P=0.001)和死亡率较低(0.41 [0.29-0.58];P<0.001)。相比之下,他汀类药物停药与功能结局不良相关(1.83 [1.01-3.30];P=0.045)。在接受溶栓治疗的患者中,他汀类药物与良好的功能结局相关(1.44 [1.10-1.89];P=0.001),尽管症状性出血性转化的风险增加(1.63 [1.04-2.56];P=0.035)。
本研究结果支持在 AIS 中使用他汀类药物。然而,这些发现主要是由存在偏倚风险的观察性研究驱动的,因此大规模的随机临床试验将提供证实性证据。