Davis William W, Mullany Luke C, Schissler Matt, Albert Saw, Beyrer Chris
Center for Public Health and Human Rights, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD USA.
Department of Anthropology, University of Michigan, Ann Arbor, MI USA.
Confl Health. 2015 Oct 6;9:32. doi: 10.1186/s13031-015-0059-0. eCollection 2015.
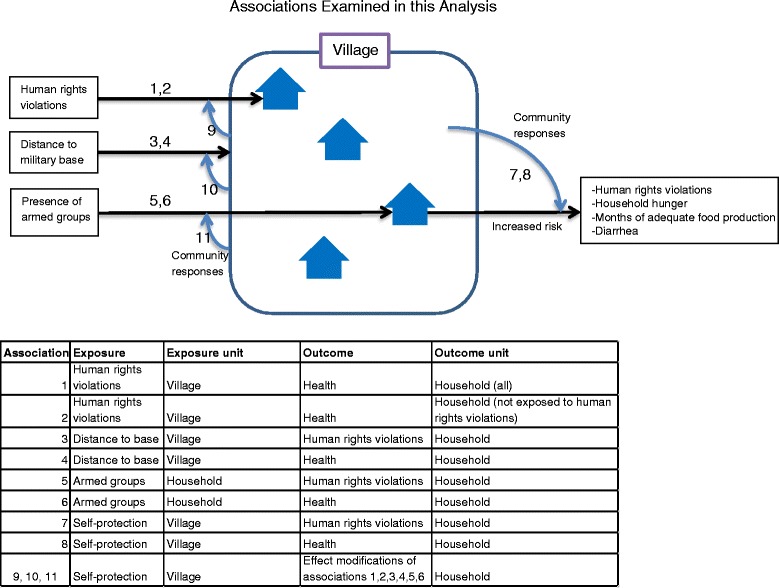
The Myanmar army and ethnic armed groups agreed to a preliminary ceasefire in 2012, but a heavy military presence remains in southeastern Myanmar. Qualitative data suggested this militarization can result in human rights abuses in the absence of armed engagements between the parties, and that rural ethnic civilians use a variety of self-protection strategies to avoid these abuses or reduce their negative impacts. We used data from a household survey to determine prevalence of select self-protection activities and to examine exposure to armed groups, human rights violations and self-protection activities as determinants of health in southeastern Myanmar.
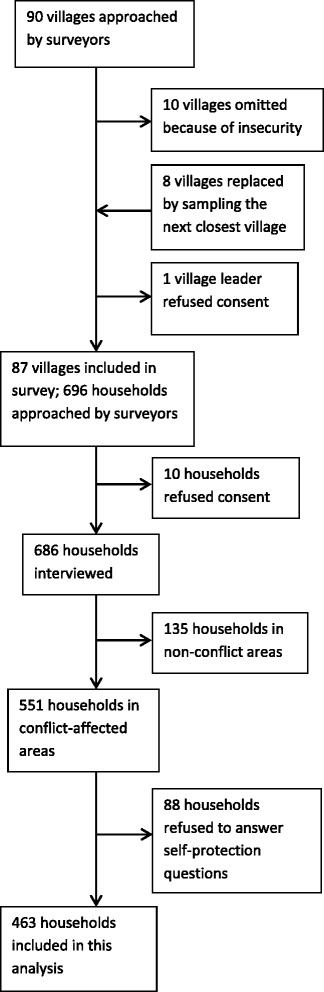
Data collected from 463 households via a two-stage cluster survey of conflict-affected areas in eastern Myanmar in January 2012, were analyzed using logistic regression models to identify associations between exposure to state and non-state armed groups, village self-protection, human rights abuses and health outcomes. Close proximity to a military base was associated with human rights abuses (PRR 1.30, 95 % CI: 1.14-1.48), inadequate food production (PRR 1.08, 95 % CI: 1.03-1.13), inability to access health care (PRR 1.29, 95 % CI: 1.04-1.60) and diarrhea (PRR 1.15, 95 % CI: 1.05-1.27. Direct exposure to armed groups was associated with household hunger (PRR1.71, 95 % CI: 1.30-2.23). Among households that reported no human rights abuses, risk of household hunger (PRR 5.64, 95 % CI: 1.88-16.91), inadequate food production (PRR 1.95, 95 % CI: 1.11-3.41) and diarrhea (PRR 2.53, 95 % CI: 1.45-4.42) increased when neighbors' households reported experiencing human rights abuses. Households in villages that reported negotiating with the Myanmar army had lower risk of human rights violations (PRR 0.91, 95 % CI: 0.85-0.98), household hunger (PRR 0.85, 95 % CI: 0.74-0.96), inadequate food production (PRR 0.93, 95 % CI:0.89-0.98) and diarrhea (PRR 0.89, 95 % CI:0.82-0.97). Stratified analysis suggests that self-protection strategies may modify the effect of exposure to armed groups on risk of human rights violations and some health outcomes.
Militarization may negatively affect health in southeastern Myanmar, and village self-protection activities may reduce these impacts. As southeastern Myanmar opens to international health and development interventions, implementing agencies should consider militarization as a determinant of health and design interventions that can mediate its effects. Such interventions should take into account existing self-protection strategies, seek to provide support where possible and, at all times, take care not to unintentionally undermine them.
缅甸军队与 ethnic armed groups 在 2012 年达成了初步停火协议,但缅甸东南部仍有大量军事存在。定性数据表明,这种军事化在各方没有武装冲突的情况下可能导致侵犯人权行为,而且农村 ethnic 平民会采用多种自我保护策略来避免这些侵犯行为或减轻其负面影响。我们利用一项家庭调查的数据来确定特定自我保护活动的 prevalence,并将接触武装组织、侵犯人权行为和自我保护活动作为缅甸东南部健康状况的决定因素进行研究。
2012 年 1 月通过对缅甸东部受冲突影响地区进行两阶段整群调查从 463 户家庭收集的数据,使用逻辑回归模型进行分析,以确定接触国家和非国家武装组织、村庄自我保护、侵犯人权行为与健康结果之间的关联。靠近军事基地与侵犯人权行为(PRR 1.30,95% CI:1.14 - 1.48)、粮食产量不足(PRR 1.08,95% CI:1.03 - 1.13)、无法获得医疗保健(PRR 1.29,95% CI:1.04 - 1.60)以及腹泻(PRR 1.15,95% CI:1.05 - 1.27)相关。直接接触武装组织与家庭饥饿(PRR1.71,95% CI:1.30 - 2.23)相关。在报告没有侵犯人权行为的家庭中,当邻居家庭报告遭受侵犯人权行为时,家庭饥饿风险(PRR 5.64,95% CI:1.88 - 16.91)、粮食产量不足(PRR 1.95,95% CI:1.11 - 3.41)和腹泻(PRR 2.53,95% CI:1.45 - 4.42)会增加。报告与缅甸军队进行谈判的村庄中的家庭,侵犯人权行为风险(PRR 0.91,95% CI:0.85 - 0.98)、家庭饥饿风险(PRR 0.85,95% CI:0.74 - 0.96)、粮食产量不足风险(PRR 0.93,95% CI:0.89 - 0.98)和腹泻风险(PRR 0.89,95% CI:0.82 - 0.97)较低。分层分析表明,自我保护策略可能会改变接触武装组织对侵犯人权行为风险和一些健康结果的影响。
军事化可能对缅甸东南部的健康产生负面影响,而村庄自我保护活动可能会减轻这些影响。随着缅甸东南部向国际卫生和发展干预开放,实施机构应将军事化视为健康的一个决定因素,并设计能够调节其影响的干预措施。此类干预措施应考虑现有的自我保护策略,尽可能提供支持,并始终注意不要无意地破坏这些策略。