Gaudard Philippe, Mourad Marc, Eliet Jacob, Zeroual Norddine, Culas Geraldine, Rouvière Philippe, Albat Bernard, Colson Pascal
Department of Anesthesiology and Critical Care Medicine, Arnaud de Villeneuve Hospital, CHRU Montpellier, 371 Avenue du Doyen Gaston Giraud, 34295, Montpellier, France.
PhyMedExp, University of Montpellier, INSERM U1046, CNRS UMR9214, 371 avenue du Doyen G. Giraud, 34295, Montpellier, France.
Crit Care. 2015 Oct 9;19:363. doi: 10.1186/s13054-015-1073-8.
Cardiogenic shock refractory to standard therapy with inotropes and/or intra-aortic balloon pump is accompanied with an unacceptable high mortality. Percutaneous left ventricular assist devices may provide a survival benefit for these very sick patients. In this study, we describe our experience with the Impella 5.0 device used in the setting of refractory cardiogenic shock.
In this observational, retrospective, single-center study we included all the consecutive patients supported with Impella 5.0, between May 2008 and December 2013, for refractory cardiogenic shock. Patients' baseline and procedural characteristics, hemodynamics and outcome to the first 48 h of support, to ICU discharge and day-28 visit were collected.
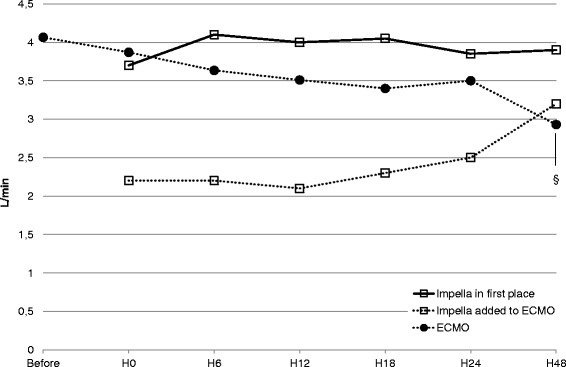
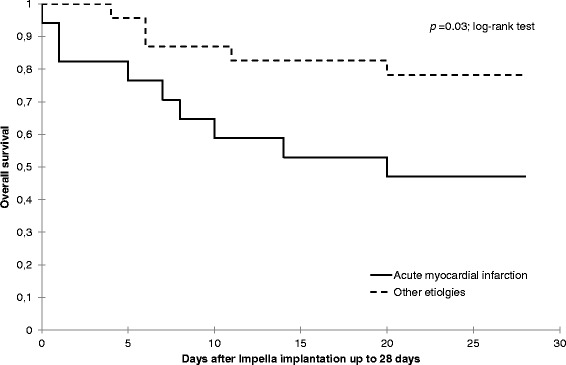
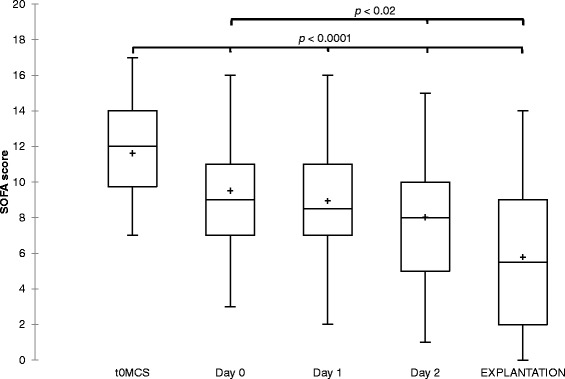
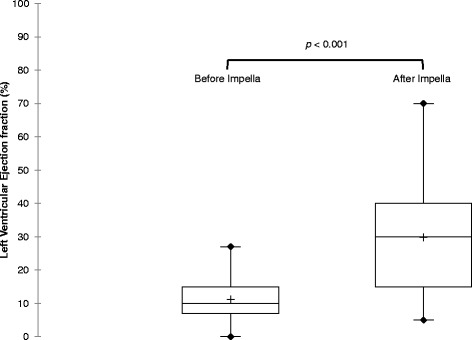
A total of 40 patients were included in the study. Median age was 57 years and 87.5 % were male. Cardiogenic shock resulted from acute myocardial infarction in 17 patients (43 %), dilated cardiomyopathy in 12 (30 %) and postcardiotomy cardiac failure in 7 (18 %). In 15 patients Impella 5.0 was added to an ECMO to unload the left ventricle. The median SOFA score for the entire cohort prior to circulatory support was 12 [10-14] and the duration of Impella support was 7 [5-10] days. We observed a significant decrease of the inotrope score (10 [1-17] vs. 1 [0-9]; p = 0.04) and the lactate values (3.8 [1.7-5.9] mmol/L vs. 2.5 [1.5-3.4] mmol/L; p = 0.01) after 6 h of support with Impella 5.0. Furthermore, at Impella removal the patients' left ventricular ejection fraction improved significantly (p < 0.001) when compared to baseline. Cardiac recovery, bridge to left ventricular assist device or heart transplantation was possible in 28 patients (70 %). Twenty-six patients (65 %) survived at day 28. A multivariate analysis showed a higher risk of mortality for patients with acute myocardial infarction (hazard ratio = 4.1 (1.2-14.2); p = 0.02).
Impella 5.0 allowed fast weaning of inotropes and might facilitate myocardial recovery. Despite high severity scores at admission, day-28 mortality rate was better than predicated.
对于使用正性肌力药物和/或主动脉内球囊反搏进行标准治疗无效的心源性休克,其死亡率高得令人难以接受。经皮左心室辅助装置可能会为这些重症患者带来生存获益。在本研究中,我们描述了在难治性心源性休克患者中使用Impella 5.0装置的经验。
在这项观察性、回顾性、单中心研究中,我们纳入了2008年5月至2013年12月期间所有连续使用Impella 5.0装置治疗难治性心源性休克的患者。收集患者的基线和手术特征、支持治疗最初48小时的血流动力学情况以及重症监护病房(ICU)出院时和第28天随访时的结果。
本研究共纳入40例患者。中位年龄为57岁,男性占87.5%。心源性休克的病因包括急性心肌梗死17例(43%)、扩张型心肌病12例(30%)和心脏手术后心力衰竭7例(18%)。15例患者在体外膜肺氧合(ECMO)基础上加用Impella 5.0以减轻左心室负荷。循环支持前整个队列的序贯器官衰竭评估(SOFA)评分中位数为12[10 - 14],Impella支持时间为7[5 - 10]天。我们观察到使用Impella 5.0支持6小时后,正性肌力药物评分显著降低(10[1 - 17]对1[0 - 9];p = 0.04),乳酸值也显著降低(3.8[1.7 - 5.9]mmol/L对2.5[1.5 - 3.4]mmol/L;p = 0.01)。此外,与基线相比,拔除Impella时患者的左心室射血分数显著改善(p < 0.001)。28例患者(70%)实现了心脏功能恢复、过渡到左心室辅助装置或心脏移植。26例患者(65%)在第28天存活。多因素分析显示,急性心肌梗死患者的死亡风险更高(风险比 = 4.1(1.2 - 14.2);p = 0.02)。
Impella 5.0能够快速撤掉正性肌力药物,并可能促进心肌恢复。尽管入院时病情严重程度评分较高,但第28天的死亡率优于预期。