Inoue Daisuke, Muraoka Ryoichi, Okazaki Ryo, Nishizawa Yoshiki, Sugimoto Toshitsugu
Third Department of Medicine, Teikyo University Chiba Medical Center, 3426-3, Anesaki, Ichihara-shi, Chiba, 299-0111, Japan.
Data Science Group, Clinical Development Department, Ajinomoto Pharmaceuticals Co., Ltd., Tokyo, Japan.
Calcif Tissue Int. 2016 Feb;98(2):114-22. doi: 10.1007/s00223-015-0071-9. Epub 2015 Oct 14.
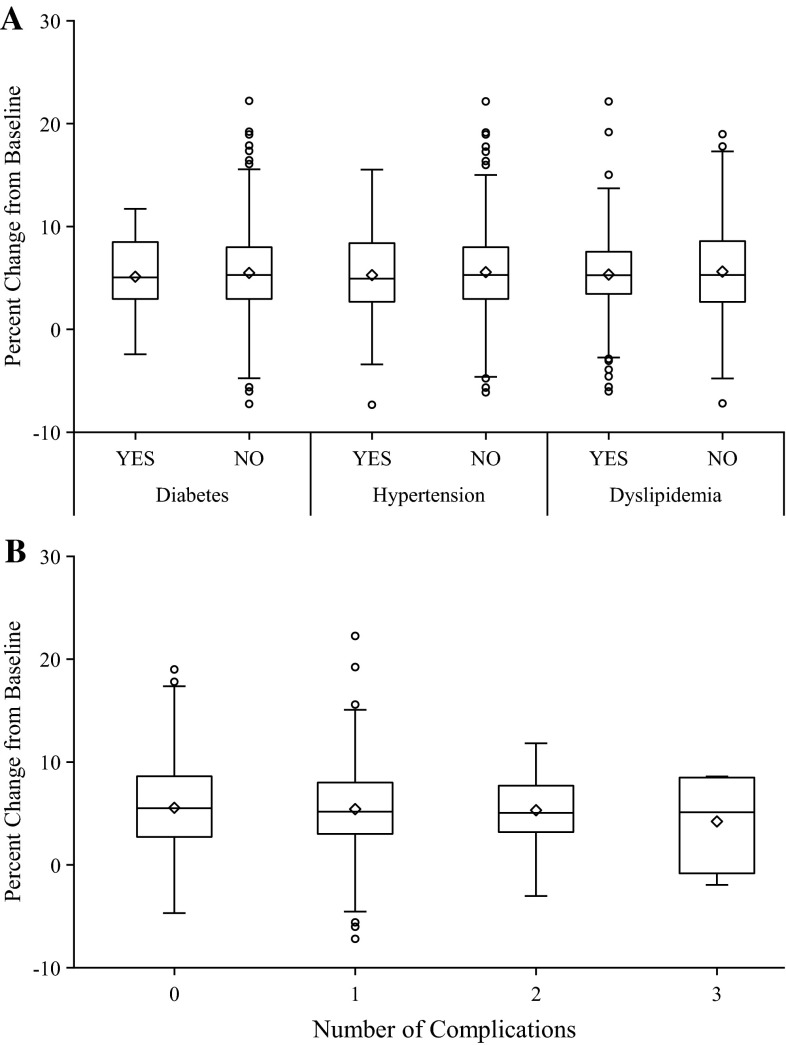
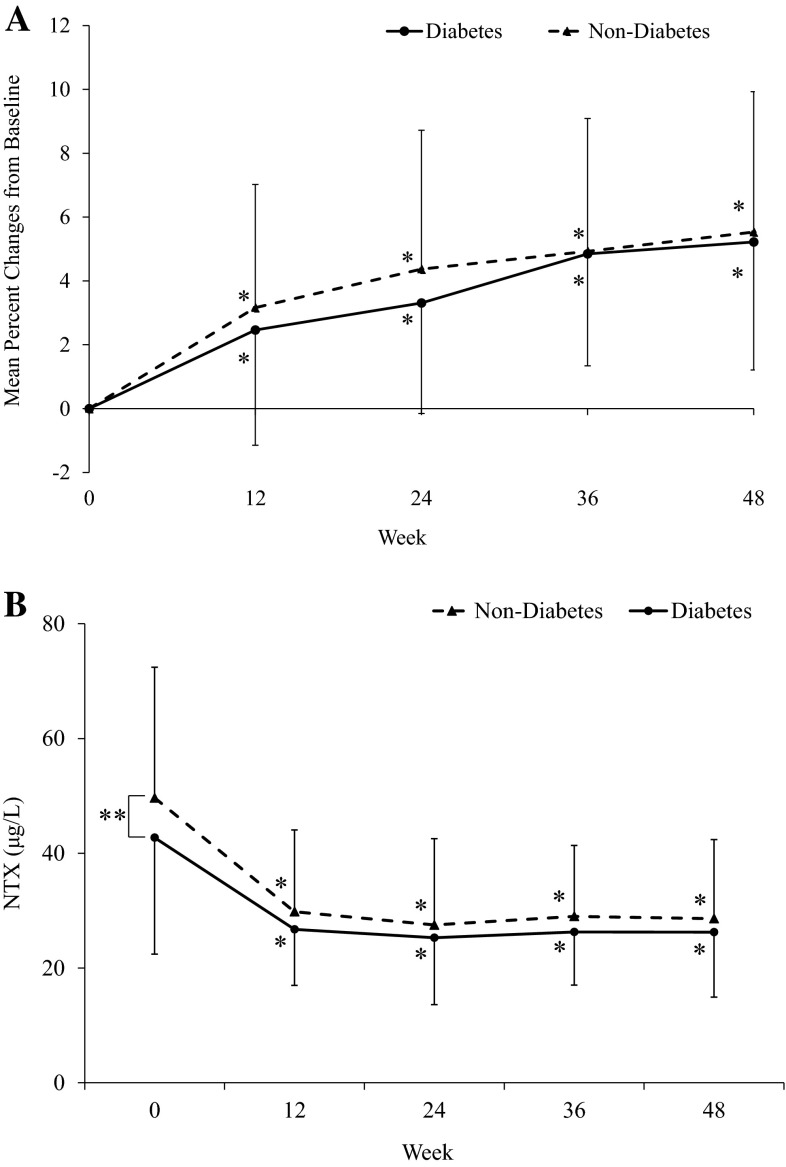
Many osteoporotics have comorbid diabetes mellitus (DM), hypertension (HT), and dyslipidemia (DL). However, whether such comorbidities alter response to anti-osteoporotic treatment is unknown. We did post hoc analyses of combined data from three risedronate Japanese phase III trials to determine whether the presence of DM, HT, or DL affects its efficacy and safety. Data from 885 subjects who received 48-week treatment with risedronate were collected and combined from the three phase III trials. They were divided into two groups by the presence or absence of comorbidities: DM (n = 53) versus non-DM (n = 832); HT (n = 278) versus non-HT (n = 607); and DL (n = 292) versus non-DL (n = 593). Bone mineral density (BMD), urinary type 1 collagen N-telopeptide (uNTX), and serum bone-specific alkaline phosphatase (BAP) were measured at baseline and sequentially until 48 weeks. BMD or bone markers were not different between any of the two groups. Overall, BMD was increased by 5.52%, and uNTX and BAP were decreased by 35.4 and 33.8%, respectively. Some bone markers were slightly lower in DM and DL subjects, but the responses to risedronate were not significantly different. Statin users had lower uNTX and BAP, but showed no difference in the treatment response. All the other medications had no apparent effect. Adverse event incidence was marginally higher in DL compared with non-DL (Relative risk 1.06; 95% confidence interval 1.01-1.11), but was not related to increase in any specific events. Risedronate shows consistent safety and efficacy in suppressing bone turnover and increasing BMD in osteoporosis patients with comorbid DM, HT, and/or DL.
许多骨质疏松症患者合并有糖尿病(DM)、高血压(HT)和血脂异常(DL)。然而,这些合并症是否会改变抗骨质疏松治疗的反应尚不清楚。我们对三项利塞膦酸钠日本III期试验的合并数据进行了事后分析,以确定DM、HT或DL的存在是否会影响其疗效和安全性。收集了三项III期试验中885名接受利塞膦酸钠48周治疗的受试者的数据并进行合并。根据是否存在合并症将他们分为两组:DM组(n = 53)与非DM组(n = 832);HT组(n = 278)与非HT组(n = 607);DL组(n = 292)与非DL组(n = 593)。在基线时及随后直至48周测量骨密度(BMD)、尿I型胶原N-端肽(uNTX)和血清骨特异性碱性磷酸酶(BAP)。两组之间的BMD或骨标志物没有差异。总体而言,BMD增加了5.52%,uNTX和BAP分别下降了35.4%和33.8%。DM和DL受试者的一些骨标志物略低,但对利塞膦酸钠的反应没有显著差异。他汀类药物使用者的uNTX和BAP较低,但治疗反应没有差异。所有其他药物没有明显效果。DL组的不良事件发生率略高于非DL组(相对风险1.06;置信区间95% 为1.01 - 1.11),但与任何特定事件的增加无关。利塞膦酸钠在合并DM、HT和/或DL的骨质疏松症患者中,在抑制骨转换和增加BMD方面显示出一致的安全性和疗效。