Williams Kirsten M, Cheng Guang-Shing, Pusic Iskra, Jagasia Madan, Burns Linda, Ho Vincent T, Pidala Joseph, Palmer Jeanne, Johnston Laura, Mayer Sebastian, Chien Jason W, Jacobsohn David A, Pavletic Steven Z, Martin Paul J, Storer Barry E, Inamoto Yoshihiro, Chai Xiaoyu, Flowers Mary E D, Lee Stephanie J
Division of Blood and Marrow Transplantation, Children's Research Institute, Children's National Health System, Washington, DC; Experimental Transplantation and Immunology Branch, National Cancer Institute, National Institutes of Health, Bethesda, Maryland.
Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, Washington.
Biol Blood Marrow Transplant. 2016 Apr;22(4):710-716. doi: 10.1016/j.bbmt.2015.10.009. Epub 2015 Oct 22.
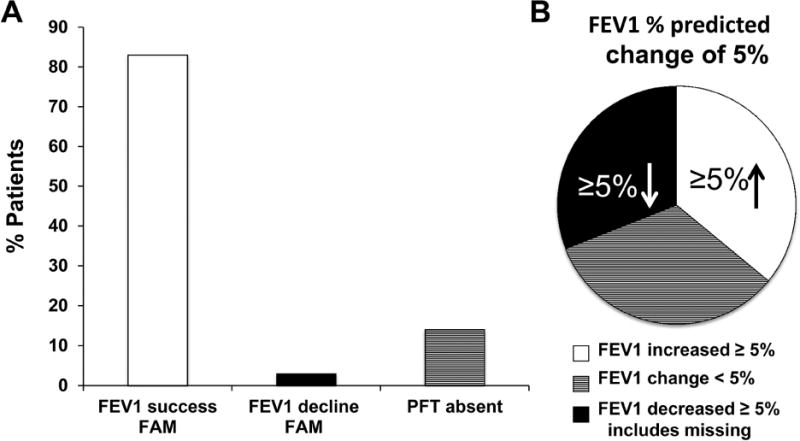
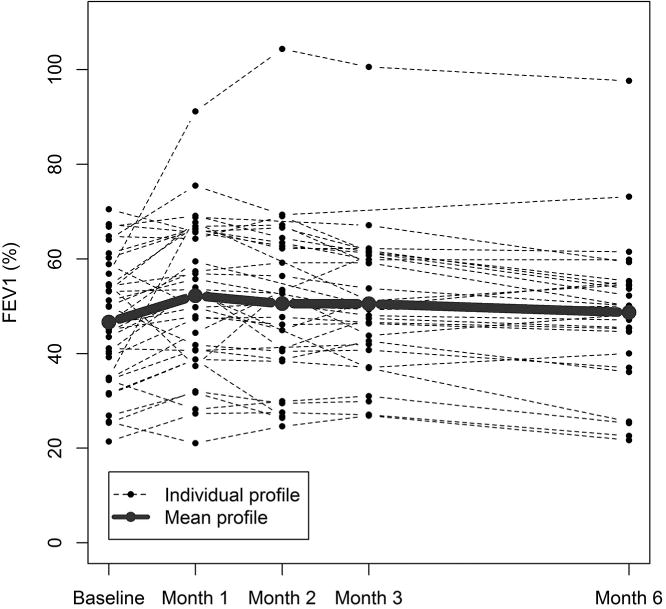
Bronchiolitis obliterans syndrome (BOS) after allogeneic hematopoietic cell transplantation (HCT) is associated with high mortality. We hypothesized that inhaled fluticasone, azithromycin, and montelukast (FAM) with a brief steroid pulse could avert progression of new-onset BOS. We tested this in a phase II, single-arm, open-label, multicenter study (NCT01307462). Thirty-six patients were enrolled within 6 months of BOS diagnosis. The primary endpoint was treatment failure, defined as 10% or greater forced expiratory volume in 1 second decline at 3 months. At 3 months, 6% (2 of 36, 95% confidence interval, 1% to 19%) had treatment failure (versus 40% in historical controls, P < .001). FAM was well tolerated. Steroid dose was reduced by 50% or more at 3 months in 48% of patients who could be evaluated (n = 27). Patient-reported outcomes at 3 months were statistically significantly improved for Short-Form 36 social functioning score and mental component score, Functional Assessment of Cancer Therapies emotional well-being, and Lee symptom scores in lung, skin, mouth, and the overall summary score compared to enrollment (n = 24). At 6 months, 36% had treatment failure (95% confidence interval, 21% to 54%, n = 13 of 36, with 6 documented failures, 7 missing pulmonary function tests). Overall survival was 97% (95% confidence interval, 84% to 100%) at 6 months. These data suggest that FAM was well tolerated and that treatment with FAM and steroid pulse may halt pulmonary decline in new-onset BOS in the majority of patients and permit reductions in systemic steroid exposure, which collectively may improve quality of life. However, additional treatments are needed for progressive BOS despite FAM.
异基因造血细胞移植(HCT)后发生的闭塞性细支气管炎综合征(BOS)与高死亡率相关。我们假设吸入氟替卡松、阿奇霉素和孟鲁司特(FAM)并给予短期类固醇冲击治疗可以避免新发BOS的进展。我们在一项II期、单臂、开放标签、多中心研究(NCT01307462)中对此进行了测试。36例患者在BOS诊断后的6个月内入组。主要终点是治疗失败,定义为3个月时第一秒用力呼气量下降10%或更多。3个月时,6%(36例中的2例,95%置信区间为1%至19%)出现治疗失败(与历史对照中的40%相比,P<0.001)。FAM耐受性良好。在可评估的患者中(n = 27),48%的患者在3个月时类固醇剂量减少了50%或更多。与入组时相比(n = 24),3个月时患者报告的结果在简短健康调查问卷36项社会功能评分和心理成分评分、癌症治疗功能评估情绪健康评分以及肺部、皮肤、口腔的李症状评分和总体总结评分方面有统计学显著改善。6个月时,36%的患者出现治疗失败(95%置信区间为21%至54%,36例中的13例,其中6例有记录的失败,7例肺功能测试缺失)。6个月时总生存率为97%(95%置信区间为84%至100%)。这些数据表明FAM耐受性良好,FAM和类固醇冲击治疗可能会使大多数新发BOS患者的肺部功能下降停止,并允许减少全身类固醇暴露,这可能共同改善生活质量。然而,尽管有FAM治疗,进展性BOS仍需要额外的治疗。