Takeuchi K, Togashi Y, Kamihara Y, Fukuyama T, Yoshioka H, Inoue A, Katsuki H, Kiura K, Nakagawa K, Seto T, Maemondo M, Hida T, Harada M, Ohe Y, Nogami N, Yamamoto N, Nishio M, Tamura T
Pathology Project for Molecular Targets Division of Pathology, the Cancer Institute, Japanese Foundation for Cancer Research, Tokyo
Pathology Project for Molecular Targets Division of Pathology, the Cancer Institute, Japanese Foundation for Cancer Research, Tokyo.
Ann Oncol. 2016 Jan;27(1):185-92. doi: 10.1093/annonc/mdv501. Epub 2015 Oct 20.
Anaplastic lymphoma kinase (ALK) fusions need to be accurately and efficiently detected for ALK inhibitor therapy. Fluorescence in situ hybridization (FISH) remains the reference test. Although increasing data are supporting that ALK immunohistochemistry (IHC) is highly concordant with FISH, IHC screening needed to be clinically and prospectively validated.
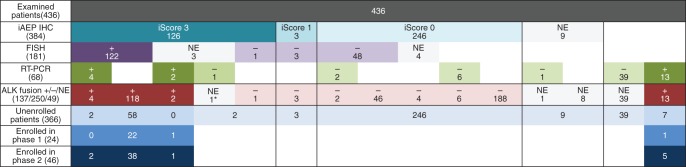
In the AF-001JP trial for alectinib, 436 patients were screened for ALK fusions through IHC (n = 384) confirmed with FISH (n = 181), multiplex RT-PCR (n = 68), or both (n = 16). IHC results were scored with iScore.
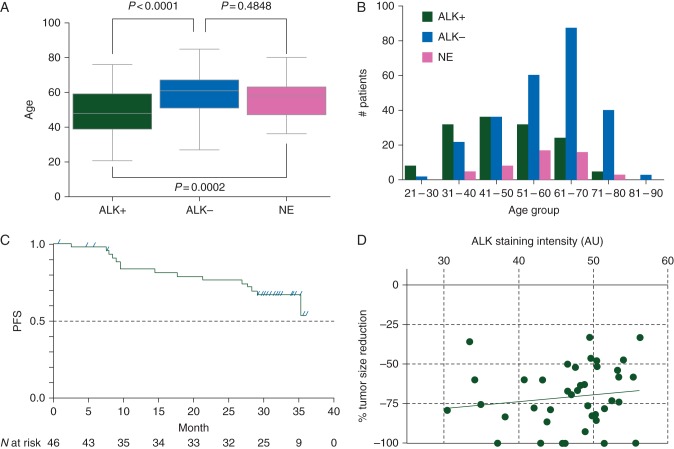
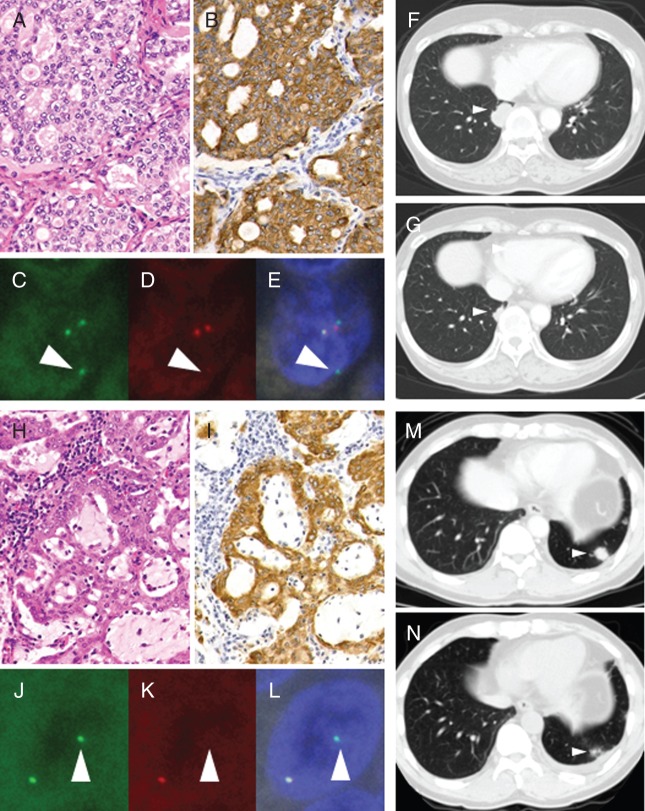
ALK fusion was positive in 137 patients and negative in 250 patients. Since the presence of cancer cells in the samples for RT-PCR was not confirmed, ALK fusion negativity could not be ascertained in 49 patients. IHC interpreted with iScore showed a 99.4% (173/174) concordance with FISH. All 41 patients who had iScore 3 and were enrolled in phase II showed at least 30% tumor reduction with 92.7% overall response rate. Two IHC-positive patients with an atypical FISH pattern responded to ALK inhibitor therapy. The reduction rate was not correlated with IHC staining intensity.
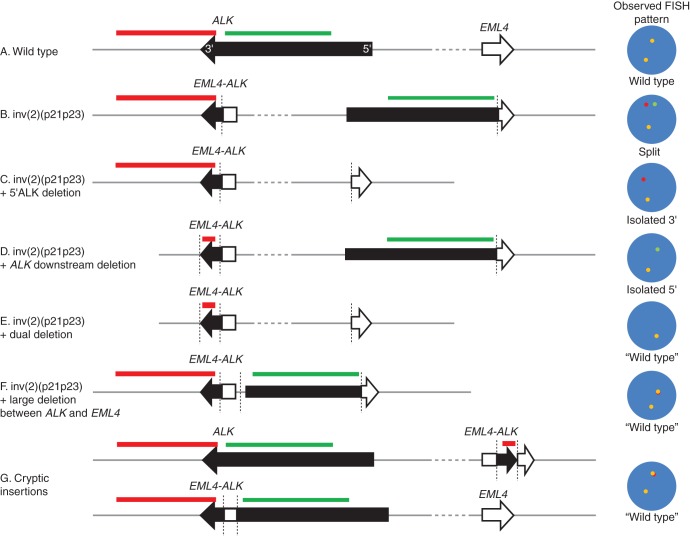
Our study showed (i) that when sufficiently sensitive and appropriately interpreted, IHC can be a stand-alone diagnostic for ALK inhibitor therapies; (ii) that when atypical FISH patterns are accompanied by IHC positivity, the patients should be considered as candidates for ALK inhibitor therapies, and (iii) that the expression level of ALK fusion is not related to the level of response to ALK inhibitors and is thus not required for patient selection.
JapicCTI-101264 (This study is registered with the Japan Pharmaceutical Information Center).
为了进行间变性淋巴瘤激酶(ALK)抑制剂治疗,需要准确、高效地检测ALK融合。荧光原位杂交(FISH)仍然是参考检测方法。尽管越来越多的数据支持ALK免疫组化(IHC)与FISH高度一致,但IHC筛查仍需进行临床前瞻性验证。
在阿来替尼的AF-001JP试验中,436例患者通过IHC(n = 384)进行ALK融合筛查,并用FISH(n = 181)、多重逆转录聚合酶链反应(n = 68)或两者(n = 16)进行确认。IHC结果采用iScore评分。
137例患者ALK融合阳性,250例患者ALK融合阴性。由于未确认用于逆转录聚合酶链反应的样本中存在癌细胞,49例患者无法确定ALK融合阴性。采用iScore解释的IHC与FISH的一致性为99.4%(173/174)。所有41例iScore为3且进入II期的患者肿瘤缩小至少30%,总缓解率为92.7%。2例具有非典型FISH模式的IHC阳性患者对ALK抑制剂治疗有反应。缓解率与IHC染色强度无关。
我们的研究表明:(i)当具有足够的敏感性并得到适当解释时,IHC可作为ALK抑制剂治疗的独立诊断方法;(ii)当非典型FISH模式伴有IHC阳性时,患者应被视为ALK抑制剂治疗的候选者;(iii)ALK融合的表达水平与对ALK抑制剂的反应水平无关,因此在患者选择时不需要考虑。
JapicCTI-101264(本研究已在日本药品信息中心注册)