Hooper Lee, Abdelhamid Asmaa, Ali Adam, Bunn Diane K, Jennings Amy, John W Garry, Kerry Susan, Lindner Gregor, Pfortmueller Carmen A, Sjöstrand Fredrik, Walsh Neil P, Fairweather-Tait Susan J, Potter John F, Hunter Paul R, Shepstone Lee
Norwich Medical School, University of East Anglia, Norwich, UK.
Norfolk and Norwich University Hospitals NHS Foundation Trust, Norwich, UK.
BMJ Open. 2015 Oct 21;5(10):e008846. doi: 10.1136/bmjopen-2015-008846.
To assess which osmolarity equation best predicts directly measured serum/plasma osmolality and whether its use could add value to routine blood test results through screening for dehydration in older people.
Diagnostic accuracy study.
Older people (≥65 years) in 5 cohorts: Dietary Strategies for Healthy Ageing in Europe (NU-AGE, living in the community), Dehydration Recognition In our Elders (DRIE, living in residential care), Fortes (admitted to acute medical care), Sjöstrand (emergency room) or Pfortmueller cohorts (hospitalised with liver cirrhosis).
Directly measured serum/plasma osmolality: current dehydration (serum osmolality>300 mOsm/kg), impending/current dehydration (≥295 mOsm/kg).
39 osmolarity equations calculated using serum indices from the same blood draw as directly measured osmolality.
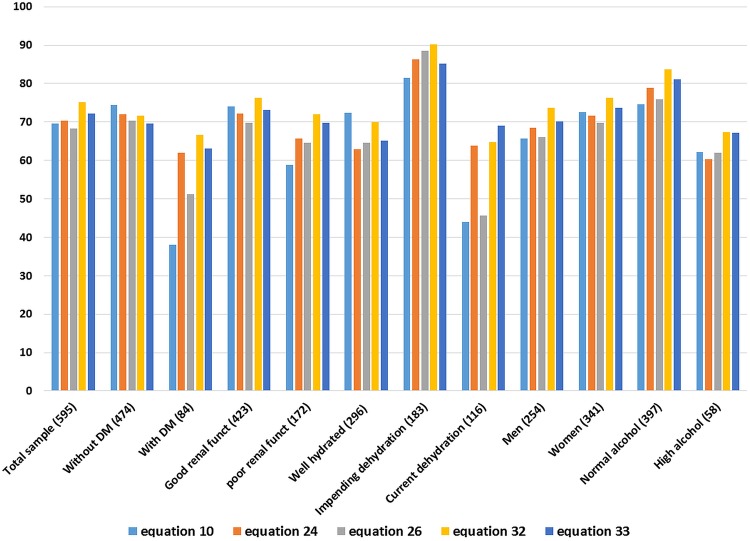
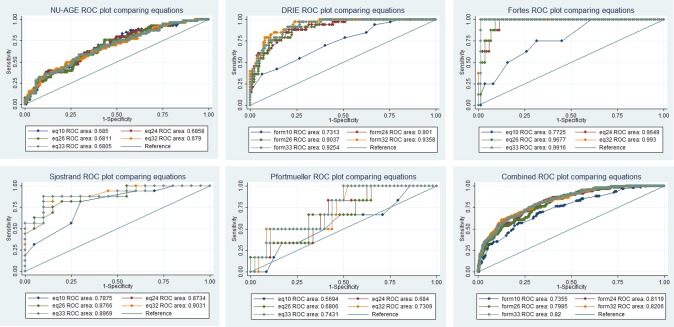
Across 5 cohorts 595 older people were included, of whom 19% were dehydrated (directly measured osmolality>300 mOsm/kg). Of 39 osmolarity equations, 5 showed reasonable agreement with directly measured osmolality and 3 had good predictive accuracy in subgroups with diabetes and poor renal function. Two equations were characterised by narrower limits of agreement, low levels of differential bias and good diagnostic accuracy in receiver operating characteristic plots (areas under the curve>0.8). The best equation was osmolarity=1.86×(Na++K+)+1.15×glucose+urea+14 (all measured in mmol/L). It appeared useful in people aged ≥65 years with and without diabetes, poor renal function, dehydration, in men and women, with a range of ages, health, cognitive and functional status.
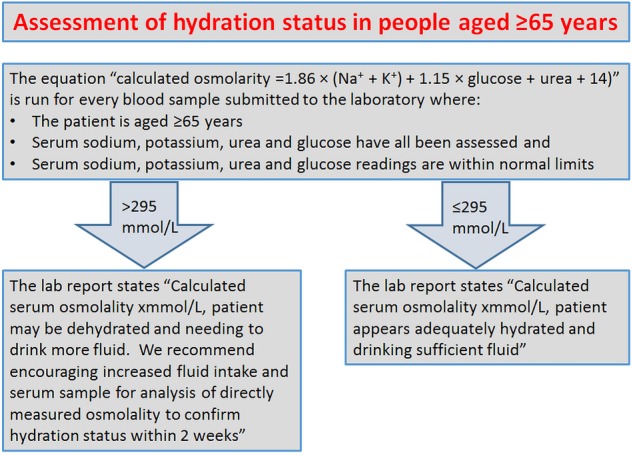
Some commonly used osmolarity equations work poorly, and should not be used. Given costs and prevalence of dehydration in older people we suggest use of the best formula by pathology laboratories using a cutpoint of 295 mOsm/L (sensitivity 85%, specificity 59%), to report dehydration risk opportunistically when serum glucose, urea and electrolytes are measured for other reasons in older adults.
DRIE: Research Register for Social Care, 122273; NU-AGE: ClinicalTrials.gov NCT01754012.
评估哪种渗透压方程能最佳预测直接测量的血清/血浆渗透压,以及其应用是否可通过筛查老年人脱水情况为常规血液检测结果增添价值。
诊断准确性研究。
来自5个队列的老年人(≥65岁):欧洲健康老龄化饮食策略(NU-AGE,居住在社区)、老年人脱水识别(DRIE,居住在养老院)、福泰斯(入住急性医疗护理机构)、舍斯特兰德(急诊室)或普福特米勒队列(因肝硬化住院)。
直接测量的血清/血浆渗透压:当前脱水(血清渗透压>300 mOsm/kg),即将发生/当前脱水(≥295 mOsm/kg)。
使用与直接测量的渗透压相同血样的血清指标计算的39个渗透压方程。
5个队列共纳入595名老年人,其中19%存在脱水(直接测量的渗透压>300 mOsm/kg)。在39个渗透压方程中,5个与直接测量的渗透压显示出合理的一致性,3个在糖尿病和肾功能较差的亚组中具有良好的预测准确性。两个方程的一致性界限较窄,差异偏倚水平较低,在受试者工作特征曲线中诊断准确性良好(曲线下面积>0.8)。最佳方程为渗透压=1.86×(Na⁺+K⁺)+1.15×葡萄糖+尿素+14(均以mmol/L为单位测量)。它似乎对≥65岁、有无糖尿病、肾功能差、脱水的人群,无论男女,在不同年龄、健康、认知和功能状态下均有用。
一些常用的渗透压方程效果不佳,不应使用。鉴于老年人脱水的成本和患病率,我们建议病理实验室使用最佳公式,以295 mOsm/L为切点(敏感性85%,特异性59%),在因其他原因对老年人测量血清葡萄糖、尿素和电解质时,机会性地报告脱水风险。
DRIE:社会护理研究注册,122273;NU-AGE:ClinicalTrials.gov NCT01754012。